February 2026 Case Challenge
Author: Dr. Brandon Barnett
Case submitted courtesy of Dr. Claudia Garces
Case History: A 49 year old male presented for evaluation and treatment of teeth #19 and #20 with the following chief complaint “My dentist said I have an infection, but it doesn’t hurt.”
Medical history: Non-contributory, ASA I
Medications: None
Allergies: NKDA
HPI: #19 RCT completed in 2020 and #20 RCT completed in 2009 both with a prior dentist. Pt reports a sinus tract of about 3 weeks duration which has partially resolved after taking Augmentin 875-125 BID for an unspecified duration.
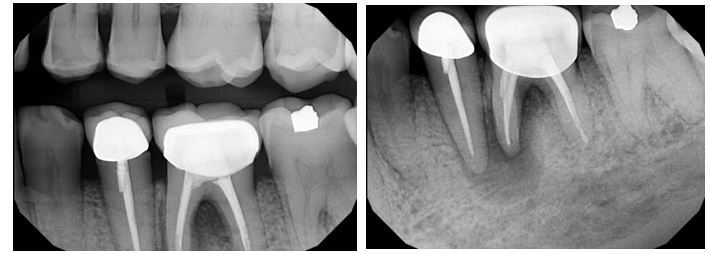
Radiographic evaluation: Periapical and bitewing radiographs of the mandibular left posterior quadrant show existing PFM crowns and prior root canal therapy on teeth #20 and #19, with a small, nonretentive post on #20. A large periapical radiolucency is noted at the M root of #19 which is confluent with a secondary large radiolucency at #20. The radiolucency on the M root of #19 extends towards the furcation.
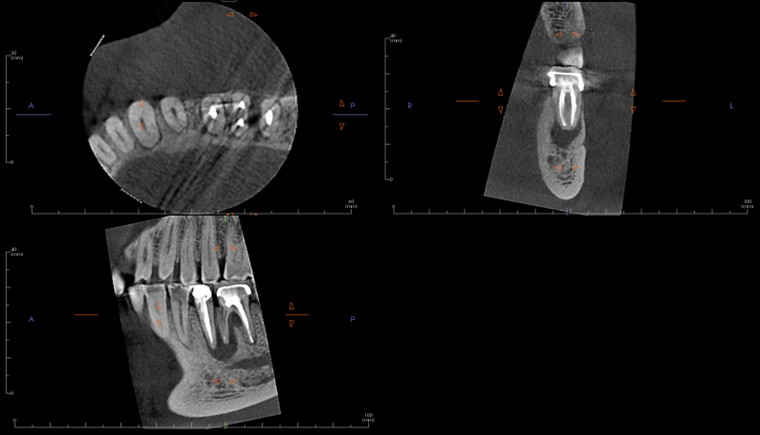
A limited FOV CBCT was exposed revealing an area of low density encompassing the root apices of #19 and #20. There was no evidence of missed/non-negotiated secondary anatomy. Existing root fills are greater than 0.5mm from the radiographic apex. The areas of reduced radiographic density are consistent with the appearance of apical periodontitis, and are not in close proximity to the inferior alveolar nerve.
Clinical evaluation: Probing depths ranged between 2-3mm in the mandibular left posterior quadrant save for the MB of tooth #19 where a probing depth of 10mm was noted. Sinus tract on the attached gingiva buccal to #19 was noted. Teeth #20 and #19 have class 1 mobility. Both PFM crowns on #19 and #20 present with clinically intact margins.
Testing:
#18 cold (+), percussion (-), palpation (-)
#19 cold (-), percussion (-), palpation (-)
#20 cold (-), percussion (-), palpation (-)
Diagnoses:
Tooth #20 Previously Treated, Asymptomatic Apical Periodontitis
Tooth #19 Previously Treated, Chronic Apical Abscess.
And now let's review the results from January's Case Challenge!:
Poll Results:
What would be your primary treatment choice?
- Non-surgical retreatment of #8 24%
- Apical surgery #8 53%
- Decompression 12%
- Non-surgical retreatment #8 with immediate apical surgery
- Non-surgical retreatment of #8 with immediate decompression 6%
- Intentional replantation #8
- Extraction #8 with replacement
- Extraction #7 and #8 with replacement 6%
- No treatment and monitor
Treatment Rendered: Sometimes we have the opportunity to combine multiple treatment strategies in complex cases. In this case, non-surgical retreatment of #8 was performed in tandem with decompression. After discussing his treatment plan with the referring GD, the patient was seen first by his GD for removal of the existing crown and placement of a long-term milled temporary crown. The patient then returned to our office for the post and gutta-percha removal with placement of intracanal calcium hydroxide. This was followed by immediate decompression of the lesion. The decompression technique used was the simultaneous needle aspiration and irrigation method described by Hoen et al. (JOE, 1990). This involves placement of two 16 gauge needles into the lesion with simultaneous aspiration and irrigation with saline (no long-term drain was used). 30ml of saline was used to irrigate the lesion until the aspirated fluid was clear.
After one month, the patient returned for follow-up and the buccal sinus was still present. The tooth was re-accessed and the calcium hydroxide was replaced. At the two month mark, the buccal sinus tract was healed, but the canal still had continued mild drainage internally. A third round of calcium hydroxide was applied and left in place for 3 months. When the patient returned (5 months after initiating treatment), evidence of healing was observed radiographically around #7 and #8. RCT #8 was completed with an MTA obturation and RMGI orifice barrier. Sufficient ferrule and peripheral tooth structure was present and another post was considered not necessary.
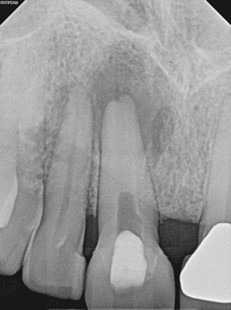
After 2 months of calcium hydroxide. Early evidence of periapical healing, The buccal sinus tract healed but the canal was still draining internally. PA taken immediately after third round of calcium hydroxide (powder) applied.
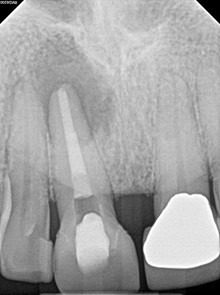
Immediate Post-op (after long-term CaOH for 5 months)
6-month recall: Tooth #8 was asymptomatic and with no buccal sinus tract present. Tooth #7 remains responsive to cold testing. The patient had not returned to their GD for the permanent crown. The mobility in #8 was notably reduced and significant healing was observed radiographically. The lesion may heal with an apical scar, but apical surgery will likely not be necessary. The patient was scheduled for a 12-month recall and advised to return to their GD soon for the permanent crown.
