Save Your Tooth Month 2026 is officially underway, and this year’s campaign is already demonstrating the power of an integrated, strategic approach to elevating the specialty of endodontics.
What began as a public awareness initiative has evolved into a multifaceted effort—one that not only educates patients on the importance of saving natural teeth, but also reinforces referral relationships with general dentists, expands visibility through corporate and media partnerships, and drives meaningful engagement at both the national and local levels.
Early results are promising. Three national news releases have already generated more than 100 million in audience reach, putting the campaign on a strong trajectory toward its ambitious goal of one billion total impressions by the end of May.
This momentum is being fueled by a robust public relations strategy designed to keep endodontics top of mind. Upcoming efforts include a satellite media tour with Dr. Noblett and an in-studio television segment at Chicago’s WGN, alongside ongoing media outreach tied to the Worth Saving message, “a healthier mouth equals a healthier you.” These initiatives are complemented by grassroots visibility efforts, including state proclamations and the Chicago Mobile Cares activation on May 12, which will bring care and education directly into the community.
Digital engagement remains a cornerstone of the campaign. Throughout the month, Endo influencers and AAE members will be featured across social media platforms, helping to humanize the specialty and expand its reach. Members are encouraged to actively engage with this content—liking, sharing, and commenting to help amplify the message and demonstrate the collective strength of the endodontic community.
Locally, progress continues to build through state-level advocacy. Proclamations recognizing Save Your Tooth Month have already been secured in Mississippi, Wisconsin, Illinois, Minnesota, Arizona, and Ohio, with additional states expected to follow. These recognitions play a key role in raising awareness and reinforcing the importance of endodontic care within communities across the country.
As Save Your Tooth Month continues, member participation remains essential. Whether through patient education, referral collaboration, media engagement, or social amplification, every effort contributes to a broader mission: ensuring patients understand that saving their natural teeth is both possible and worth it.
To learn more about campaign activities and find ways to get involved, visit aae.org/isaveteeth.
When Dr. W. Craig Noblett reflects on his path to leadership, one theme rises above the rest: collaboration. Over decades of service in organized dentistry, academia, and clinical practice, he has developed a leadership style rooted not in directive authority, but in bringing people together.
“I’ve come to realize how important it is to build a consensus among the members of your group,” he says. “So that everybody is on board with decisions that are made.”
That philosophy now guides him as he steps into his role as President of the American Association of Endodontists.
A Career Shaped by Service and Experience
Dr. Noblett’s leadership journey has been anything but linear. A graduate of the UCLA School of Dentistry, he earned his master’s degree and certificate in endodontics from the University of Iowa before building a career that spans private practice, hospital dentistry, and academia.
Along the way, he has served as president of multiple organizations, including the Berkeley Dental Society and the Northern California Academy of Endodontics, and held leadership roles with the California Dental Association and the American Board of Endodontics.
“I have a pretty good mix of different leadership roles,” he says, reflecting on years of involvement across organized dentistry.
Today, he serves as Director of the Division of Endodontics and Graduate Program Director at the University of Minnesota School of Dentistry—roles that continue to shape his perspective as both an educator and leader.
An Unexpected Path to Endodontics—and Academia
Interestingly, neither endodontics nor teaching were part of Dr. Noblett’s original plan.
“If you told me when I graduated from dental school that I was going to end up being an endodontist, I would have laughed all the way out the door,” he says.
Initially interested in oral surgery, his path shifted during a general practice residency at Northwestern Memorial Hospital, where he found himself performing more root canals than anticipated. That exposure sparked a growing interest that ultimately led him into the specialty.
His journey into academia followed a similarly organic trajectory.
“I never came into this thinking I would be teaching ever, let alone full-time,” he says. “I always thought my strength was a one-on-one patient care clinical practice.”
Yet teaching opportunities continued to present themselves throughout his career, eventually leading him to full-time academia—a transition made easier by years of consistent part-time involvement.
Shaping the Next Generation
As an educator, Dr. Noblett is deeply focused on preparing residents not just to perform procedures, but to think critically and act ethically.
“I think some of the biggest priorities for me are to teach our students to be independent thinkers and problem solvers,” he says.
Equally important is instilling a strong ethical foundation.
“I try to instill in them… ethical behavior—ethical treatment of their patients,” he explains, noting that leading by example is key.
This emphasis reflects his broader belief that the future of the specialty depends on clinicians who can navigate complexity with both skill and integrity.
Innovation with Intention
From emerging technologies to evolving treatment philosophies, Dr. Noblett sees tremendous opportunity in the future of endodontics—but he also emphasizes thoughtful adoption.
“You need to put technology to work for you rather than you working for it,” he says of new technologies.
Rather than chasing trends or succumbing to peer pressure, he encourages practitioners to critically evaluate whether innovations align with their practice philosophy and standards of care.
“Don’t try to make it fit if it doesn’t seem to fit naturally,” he adds.
At the University of Minnesota, he is helping lead research into groundbreaking advancements such as dental MRI technology—an innovation that could transform diagnostic capabilities by allowing clinicians to visualize soft tissue, including potentially the pulp itself.
“That’s going to be our Holy Grail,” he says.
Advocacy and Engagement: A Call to Action
For Dr. Noblett, involvement in organized dentistry is not optional—it’s essential.
“If you’re not at the table, you’re going to be on the menu,” he says.
He stresses the importance of ensuring that endodontists have a voice in shaping the policies and regulations that impact the profession.
“If we don’t take care of our profession, someone else is going to do it for us,” he says.
This belief is already influencing how he mentors residents, encouraging them to engage in advocacy early in their careers through experiences like legislative visits and organized dentistry initiatives.
Priorities for the Year Ahead
As AAE President, Dr. Noblett is focused on two key areas.
First, maintaining strong momentum in advocacy.
“We need to stay on top of that… we need to be aware and we need to be engaged,” he says, referencing the importance of monitoring legislative activity and strengthening grassroots involvement.
Second, addressing a growing challenge within the specialty: the shortage of full-time educators.
“If we don’t start cultivating new educators… we’re going to run out of endodontists at some point,” he warns.
He hopes to identify and address the barriers that discourage endodontists from pursuing academic careers—ensuring the sustainability of training programs and the specialty itself.
Rooted in Mentorship and Balance
Dr. Noblett credits much of his success to early influences, especially his parents.
“My dad is a general dentist… that’s where my interest in dentistry came from,” he shares, noting the impact of working in his father’s practice.
His mother, a teacher and active volunteer, helped shape his commitment to education and service.
Beyond dentistry, he values time spent traveling, practicing photography, and enjoying life with his golden retriever, Wrigley—a nod to his years in Chicago. Looking ahead, he even has plans for a post-retirement pursuit.
“I am planning on getting my sommelier certification when I retire,” he says.
A Collaborative Vision Forward
As he begins his presidency, Dr. Noblett brings a steady, thoughtful approach shaped by decades of experience—and a clear belief in the power of collaboration.
Whether advancing advocacy, strengthening education, or guiding innovation, his focus remains the same: bringing people together to move the specialty forward.
And in that sense, his leadership philosophy is as practical as it is enduring—build consensus, and progress will follow.
Dr. Noblett with his mom and dad at graduation
Dr. Noblett with Wrigley

Dr. Noblett and residents at a hockey game

With residents at APICES 2025
Elisabeth Lisican is assistant director of communications & publishing for the AAE.
By Drs. Samuel Kratchman and Andrew Grinsell
The technique of drawing blood from a patient and centrifuging platelet-rich fibrin (PRF)(1) has been used in dentistry for some time, mostly in the periodontal and oral surgery specialties, where it is commonly used for sinus lifts or ridge preservation/augmentation for eventual implant placement (2-4). In medicine, a very popular method designed to speed healing is to draw the patient’s blood, centrifuge it in a test tube with additives that prevent clotting, and produce platelet-rich plasma (PRP), which can then be injected directly into the wounded muscle, ligament, or tendon to reduce inflammation and speed up healing. At the University of Pennsylvania, we have been studying the incorporation of PRF into endodontic microsurgery, along with using the piezotome to remove a bone window (lid), and then crush that bone to be mixed with the serum of the PRF membrane, creating autogenous “sticky” bone, which is then placed back into the osteotomy site along with the PRF graft and covered by the PRF membrane.
All dentists agree that the very best types of grafts are autogenous, meaning derived from the patient (5, 6). These are better than allografts, that is, from the same species, for example, cadaver grafts, which lose their osteogenic properties due to processing. Next are xenografts, which are animal-derived, such as bovine or porcine, and have a greater chance of rejection by the recipient. Finally, alloplasts are synthetic bone and have no osteogenic properties.
The process of harvesting PRF is simple; the patient has two vials of blood drawn (four vials if the lesion is very large) into test tubes that have no additives, such as anticoagulants, and spun in a centrifuge at 2700 rpm for 12 minutes. The vials need to be counterbalanced and of equal volume when spun. The only time constraint is that the blood should be gently inverted a few times and placed in the centrifuge within 90 seconds. After the PRF is spun out in 12 minutes, you can take your time removing the PRF, cutting off the blood clot and then pressing the PRF into plugs (graft) and flattening into a membrane. These can be left in the Expression Kit (BioHorizons, Birmingham, AL, USA) throughout the surgery or placed into small metal basins and kept hydrated with serum derived from pressing the membrane. After the bioceramic root-end filling (EndoSequence Fast-set putty; Brasseler USA; Savannah, Georgia) is placed, the PRF plugs are placed into the osteotomy site and covered by the PRF membrane.
For every endodontic surgery, an osteotomy must be made or enlarged to gain access to the roots. For years, this has been accomplished by burs in a high-speed handpiece, where the bone is obliterated by the burs. With the advent of the piezoelectric unit, we can now create a bony window (lid), preserve the window in a solution such as Hanks Balanced Salt Solution (HBSS), and then, after the root-end filling is complete, replace the window and secure it into place. This is an excellent opportunity to preserve the bone, but it can be time-consuming, technique-sensitive, and difficult to secure back into place, especially if the osteotomy is altered after bone window (lid) removal. Many preoperative measurements from the CBCT need to be made, the bone needs to be removed in one piece, and if it is not securely repositioned, it can become dislodged and cause a foreign body reaction in the vestibule near the surgical site. These limiting factors have led to the concept of crushing the bone window, mixing the bone particles with the serum derived from the PRF to create “sticky bone,” and placing it back into the osteotomy before closure. This eliminates the need for many preoperative measurements, as all that matters is that the bone window is initiated 3 mm from the apices of the roots being resected. The piece of bone can come out in pieces, eliminating the often difficult part of the procedure, as the fragments of bone are crushed before being replaced at the site. Perhaps the most important reason for the bone crushing procedure is that when we traditionally cut out a window/lid, we are actually severing the blood supply to that bone, and when we reposition, we place a graft inside the osteotomy and collagen around the periphery of the window to secure it and cover it with a membrane before suturing. All chances of revascularization of this bony lid are delayed; therefore, this piece of bone maintains the space until healing can occur. The benefit of crushing the bone, mixing it with serum containing growth factors and stem cells, and placing it back into the osteotomy site sandwiched between pieces of PRF plugs and covered by a PRF membrane is that it is an autogenous graft with little to no chance of rejection and contains many progenitor cells that speed up healing.
With these new advances in endodontic microsurgery, we are taking an already successful procedure and increasing the potential for healing and reforming healthy, vital bone. More studies need to be conducted, and many more cases utilizing these techniques need to be performed and followed up carefully with 3D imaging, but the future is promising (7, 8).
Courtesy: Dr JouJou Nguyenphuc
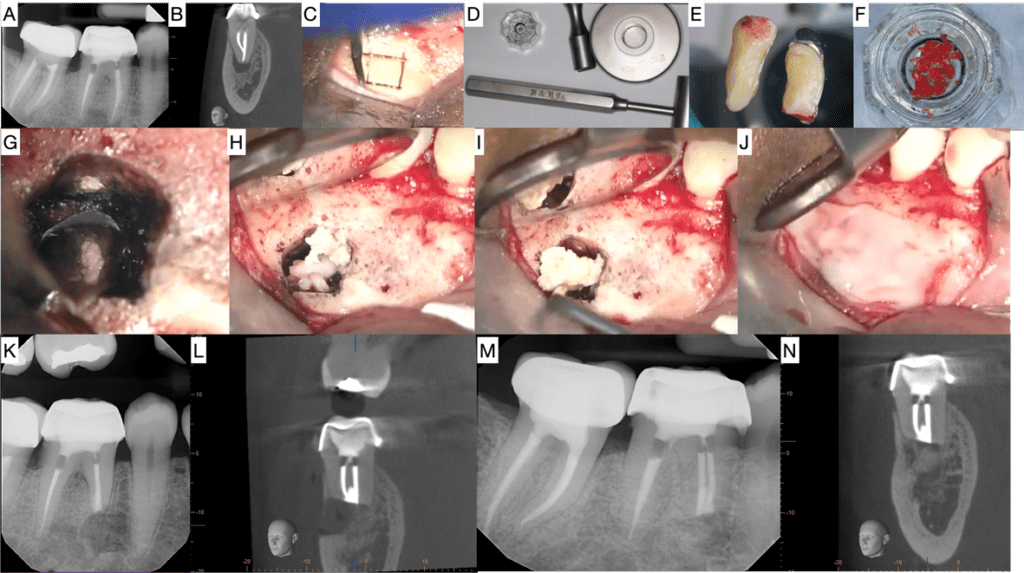
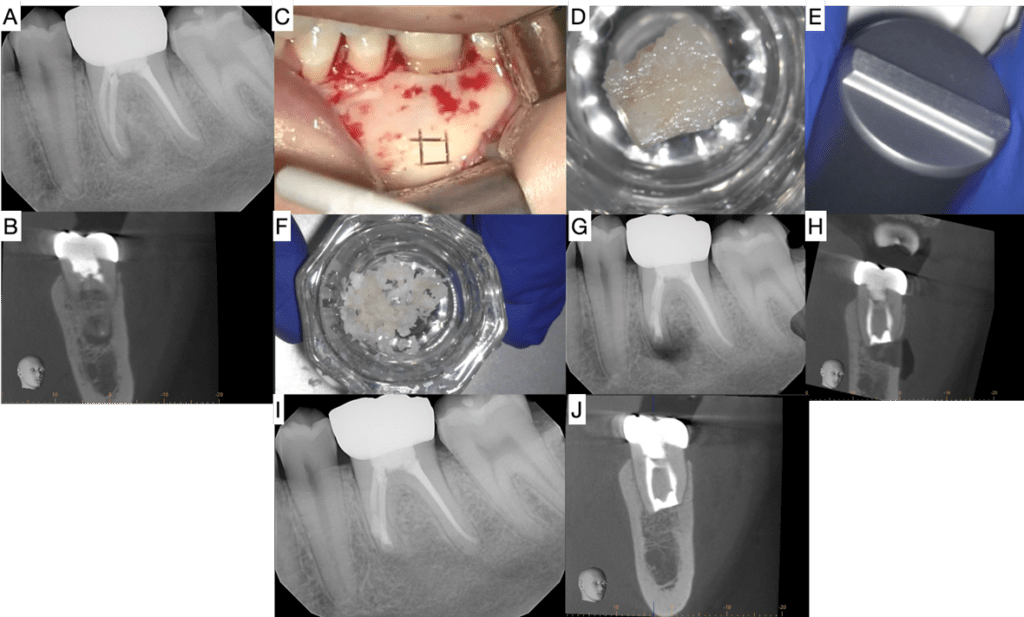
Figure 1. 55 year old female for surgery #30. A) Pre-op PA image shows PARL associated with mesial root. B) Coronal view of Pre-op CBCT showing associated low density area. C) Bone window being removed during surgery. D) Bone Crusher kit from H&H. E) L-PRF extracted from patient’s blood. F) Crushed bone mixed with L-PRF Serum (not from the case shown). G) BC putty placed. H) L-PRF graft with crushed bone. I) Crushed bone placed into osteotomy. J) L-PRF Membrane placed over osteotomy. K) Post-op PA image. The outline of the bone window is noticeable. L) Coronal view of Post-op CBCT. M) 12 month follow up PA showing complete healing. N) Coronal view of 12 month follow up CBCT showing complete cortical plate regeneration. Some bone particles are noted in the apical area.
Courtesy: Dr Jawad Jaghab
Figure 2. 25 year old female for surgery #19: A) Pre-op PA image showing PARL associated with the mesial root. B) Coronal view of Pre-op CBCT. C) Bone window cut. D) Bone window placed in dish. E) End of Bone Crusher plug, highlighting the ridge that disperses force to crush bone into fine particles. F) Bone after crushed. G) Post-op PA. H) Coronal view of Post-op CBCT. I) 12 month follow up PA showing complete healing of the mesial root. J) Coronal view of 12 month follow up CBCT showing complete regeneration of cortical plate, PDL, and Lamina dura around the mesial root.
Reference:
- Jia K, You J, Zhu Y, Li M, Chen S, Ren S, et al. Platelet-rich fibrin as an autologous biomaterial for bone regeneration: mechanisms, applications, optimization. Front Bioeng Biotechnol 2024;12:1286035.
- Castro AB, Meschi N, Temmerman A, Pinto N, Lambrechts P, Teughels W, et al. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J Clin Periodontol 2017;44(2):225–234.
- Castro AB, Meschi N, Temmerman A, Pinto N, Lambrechts P, Teughels W, et al. Regenerative potential of leucocyte- and platelet-rich fibrin. Part A: intra-bony defects, furcation defects and periodontal plastic surgery. A systematic review and meta-analysis. J Clin Periodontol 2017;44(1):67–82.
- Meschi N, Castro AB, Vandamme K, Quirynen M, Lambrechts P. The impact of autologous platelet concentrates on endodontic healing: a systematic review. Platelets 2016;27(7):613–633.
- Acocella A, Bertolai R, Colafranceschi M, Sacco R. Clinical, histological and histomorphometric evaluation of the healing of mandibular ramus bone block grafts for alveolar ridge augmentation before implant placement. J Craniomaxillofac Surg 2010;38(3):222–230.
- Aoki N, Kanayama T, Maeda M, Horii K, Miyamoto H, Wada K, et al. Sinus Augmentation by Platelet-Rich Fibrin Alone: A Report of Two Cases with Histological Examinations. Case Rep Dent 2016;2016:2654645.
- Sabeti M, Gabbay J, Ai A. Endodontic surgery and platelet concentrates: A comprehensive review. Periodontol 2000 2025;97(1):308–319.
- Rebimbas Guerreiro S, Marto CM, Paula A, Pereira JRA, Carrilho E, Marques-Ferreira M, et al. Platelet-Rich Plasma and Platelet-Rich Fibrin in Endodontics: A Scoping Review. Int J Mol Sci 2025;26(12).
The authors can be reached at sikratch@comcast.net.
Disclaimer
The views and opinions expressed by authors are solely those of the authors and do not necessarily reflect the official policy or position of the American Association of Endodontists (AAE). Publication of these views does not imply endorsement by the AAE.
By Lisa Radman White
If you are joining a private practice with the goal of pursuing a partnership, you need more information than someone who is just accepting a job. Business partnerships are like marriages, so it’s important to choose wisely. If you and your potential future partner are having open, detailed conversations about what matters most to each of you, your chances of success increase dramatically. Some important questions to consider are:
- Will you be offered an equal partnership?
- How long should you be an associate prior to partnership?
- How and when will the price be set for the partnership?
- What is the Covenant Not to Compete?
- What insurances are accepted, and what are the reimbursement rates?
- What is the exit plan if this arrangement doesn’t work out?
It is essential to have clear answers to these questions so that you understand whether the opportunity truly aligns with your goals. If a practice owner plans to bring you on with a path to partnership, take the time to ensure it is the right fit for you.
- Radman, White & Associates feels strongly that partnerships should be equal so that everyone is on the same level. It rarely makes sense to buy a fraction of a practice, as you want to be equal partners. If you are purchasing less than an equal amount then you are purchasing profit sharing. That might put more profits in your bank account, but it would likely be very challenging to sell. Most people do not want minority ownership in a practice.
- A minimum of one year together gives you a clear sense of whether you want to (or don’t want to) move forward. A timeframe greater than three years is excessive in our opinion, and benefits the owner significantly. Eighteen months to two years is what we have found to be the sweet spot for an associate period and would be a fair arrangement for everyone.
- Most often, the price for partnership should be established prior to you picking up a handpiece. The main reason is that you don’t want to spend time marketing yourself and growing the practice, only to realize that you are increasing the purchase price you will eventually pay. You shouldn’t have to pay for the growth you contributed to the practice. If there is a substantial queue of patients and you will not be required to grow the practice, then it likely makes sense to set the price after the backlog of patients has been handled. Usually, this price is set after you have been with the practice for six months, possibly a year. Even though the partnership is in the future, you should absolutely have access to the tax returns for the last three years so that you can understand the profitability of the practice.
- When we value a practice, we set the price so that the purchaser is expected to take home associate type wages after paying the overhead and the debt required to own the practice. At a minimum, you should be able to take home 40 percent, sometimes over 50 percent, while paying off the debt and expenses. While most banks loan on a 10- or 15-year term, we like to be conservative and usually examine the numbers based on a 7-year payback.
- A CNTC should cover the area around the practice that generates approximately the top 85 percent of referrals. It should not include other offices that might be opened. Rather, it is in place to protect the current referrals and the practice as it stands today, which is reasonable and fair. In most states, these CNTC’s are still enforceable. Before you join a practice in the exact place you want to be long term, you need to consider the implications of this CNTC, should this arrangement not work out.
- At a minimum, you want to ensure that the practice you are joining doesn’t accept plans that reimburse at a low rate. You don’t want to be committed to doing work at a rate far below market. For example, we once saw a situation where an endodontist brought in an associate, added plans for the associate, but stayed all fee-for-service for himself. This is not the type of partner I would want.
- You enter the practice with the intention of everything working out. However, what if you completely misjudged the situation? How do you get out? We include a 30-day notice clause for both the practice and the associate. No one should be forced to work somewhere that isn’t a fit, and this clause allows you to give notice and move elsewhere quickly.
While these are all important considerations, the absolute nonnegotiable is that you and the endodontist you are considering joining are compatible. Do you both agree that quality comes first? Do you both agree about how patients and staff should be treated? If the two of you do not have aligned work ethics, this is not the practice, nor the partnership for you. Unless there is a shared philosophy, we cannot recommend that you move forward.
Partnerships can be incredible. Partnerships provide someone to collaborate with, share overhead with, and bring different strengths to the table. The office can be covered while you are out, allowing both partners to step away when needed while maintaining a structure that can be very satisfying overall. Just remember: a partnership is like a marriage, and you certainly wouldn’t marry someone you don’t mesh with. So, gather as much information as you can before making that commitment.
Lisa Radman White is the president of Radman, White & Associates, Inc., a firm dedicated exclusively to endodontic practice transitions. The company was founded in 1998 after her father discovered firsthand how difficult it was to sell his endodontic practice as the transition market did not understand an endodontic practice. Radman, White specializes in endodontic transitions.
 By Dr. Priscilla L. Carpenter
By Dr. Priscilla L. Carpenter
What an incredibly energizing month it’s been for our endodontic community!
I want to start by recognizing the incredible engagement we saw with this year’s MTA March Madness. With 131 participants, the enthusiasm and participation were outstanding. Congratulations to our three winners, who took home gift cards of $400, $200, and $100, well deserved! If you missed out this year, be sure to join us next March for another opportunity to test your basketball knowledge and compete with colleagues across the country.
We also just wrapped up an amazing week at AAE26 in Salt Lake City (April 15–18), and it truly did not disappoint. There’s something special about being in a room filled with colleagues, mentors, faculty, and friends who are all so passionate about what we do. From outstanding lectures to fun social events, it was a perfect mix of learning, reconnecting, and making new memories. These meetings are such a reminder of how strong and supportive our community is, and honestly, they’re just a great time.
If you’re already missing it like I am, don’t worry, next year’s meeting will be in San Antonio from April 14–17, 2027. Start planning now, it’s always worth it.
In addition, we’re excited for APICES, coming up August 14–15 in St. Louis. APICES continues to be an excellent opportunity for residents and new practitioners to connect, learn, and grow within the field. We look forward to seeing many of you there.
Thank you all for your continued involvement and commitment to advancing endodontics. It’s the collective energy of this group that makes these initiatives, and our specialty, so impactful.
Until next time,
Priscilla L. Carpenter, D.D.S., M.S.
Resident and New Practitioner Committee Chair
By Dr. Jessica Hwang
Dr. Jeremy Sprouse is a second-year resident at University of Texas, Health Science Center at Houston. The Paper Point’s Dr. Jessica Hwang (PGY2, UCLA) spoke with him about his experience volunteering with the AAE Foundation through an international access-to-care trip to St. Lucia. Dr. Sprouse provided endodontic care with his mentor, Dr. Bruce Justman, at clinics in St. Lucia in partnership with Great Shape! Inc. and the Foundation’s Resident Expert Advisory Council (REACH).
1. What initially motivated you to participate in an international access-to-care mission, and can you share how this opportunity to volunteer in St. Lucia and the Foundation arose?
My motivation for participating in this international access-to-care mission is rooted in both my background and my training. Throughout my path in dentistry, I’ve seen how profoundly access, or the lack of it, shapes oral health outcomes. Even within our own communities, patients often present with severe carious lesions simply because they didn’t have the opportunity to seek care earlier or they did not have the funds to pay for the necessary treatment. As an endodontics resident, I’ve been trained to save teeth. But that skillset only has meaning if patients have access to it. This opportunity came through the AAE Foundation, whose commitment to expanding access and supporting outreach efforts made this experience possible. When the chance to serve in St. Lucia arose, it felt like a natural extension of why I chose this specialty, to provide care that preserves function, alleviates pain, and, in many cases, changes the trajectory of a patient’s oral health.
2. What types of cases were most commonly encountered during the mission, and how did they compare to what you typically see in your residency clinic?
We mostly encountered cases of extremely symptomatic irreversible pulpitis or pulpal necrosis, often in teeth that had been untreated for extended periods. While these diagnoses are familiar from residency, the key difference was in the patient presentation. Many patients came in at a much later stage of disease progression, whereas at UT Health Houston School of Dentistry, some (not an overwhelming majority) patients may present at early stages of disease progression. In addition, for some of the St. Lucian patients, this was their first time visiting a dentist, let alone receiving endodontic care. In my residency program, the patients have typically visited their general dentists before and have had one to a few root canals performed in the past. That shift in context changed my approach; I’m not only managing pathology but also intervening at a critical point to preserve teeth that might otherwise be lost. The ministry of health volunteers expressed that only a very small number of providers performed root canals on the island, and often at unaffordable prices. Furthermore, much of our treatment was performed in anterior and premolar teeth, which patients consistently identified as most important. In conversations, many explained that in a hospitality-driven workforce on the island, a person’s smile can significantly influence job prospects, often serving as a gateway to opportunities that might not otherwise be accessible.
3. Were there any particularly challenging or memorable cases that stood out to you from a clinical or emotional standpoint?
Honestly the entire experience stood out, not really for the clinical complexity of the cases, but for the stories of the patients behind them. I treated patients of all ages, but there was one young patient, in particular who had never been to a dentist before. He approached the experience with a mix of nervousness and curiosity, asking about every instrument before we even began. Another older patient shared how he fractured his anterior teeth in a motorcycle accident, and how he’s been in pain, and limited his employment opportunities, highlighting how closely oral health is tied to quality of life. We performed NSRCT on #7-10 with build ups and he left the clinic smiling, with the support of the entire community behind him. Another impactful moment involved a mother who had spent the entire day at the clinic with multiple generations of her family. After we were able to save teeth that were essential for function, she became emotional and expressed how rarely she has the chance to care for herself. Experiences like these reinforce that behind every diagnosis is a person, a story, and often, a much larger impact than we initially see.
4. I heard there were some unexpected challenges along the way and that the team adapted despite some unforeseen circumstances—how did limitations in resources, equipment, or time influence your treatment planning and decision-making?
This service trip required a high level of adaptability on different fronts. Working with limited resources, without a microscope, and within a high temperature and high-volume setting, meant that efficiency and sound clinical judgment were essential. Some of our supplies were held at sea for a few days, requiring us to use and do whatever we could to help the patients. Also, this was the first trip that the Sandals and AAE Foundations sponsored in St. Lucia for endodontics, and required logistics early on. The cases only reinforced the importance of fundamentals, access design, tactile awareness, and a strong understanding of root canal anatomy. Without relying on advanced technology such as a Cone Beam Computed Tomography (CBCT), those core principles became even more critical. Treatment planning also required sincere thoughtfulness and attention to the patient’s diagnosis, prognosis, and necessary treatment.. We had to weigh ideal treatment against what was feasible, making decisions that prioritized long-term benefit while respecting the constraints of time and resources.
5. What endodontic techniques or principles proved especially valuable in a mission-based environment?
The most valuable takeaway was that strong fundamentals and patient management translate across any environment. Careful access, effective irrigation, and efficient instrumentation were essential, particularly in the absence of advanced magnification. The ability to complete treatment in a single visit, when appropriate, also proved highly beneficial given the setting. More broadly, this experience reinforced that successful endodontics is grounded in principles and decision-making, tons of irrigation, not solely in technology.
6. What was the most rewarding aspect of participating in this mission, both professionally and personally?
Professionally, the most rewarding aspect was applying my training in a setting where the impact was immediate and meaningful. The people of St. Lucia were extremely kind, appreciative, and friendly. It felt nice to give back and I am extremely grateful for the opportunity from the AAE Foundation and certainly look forward to potentially serving as a mentor in the future. Personally, it was the connection with patients and having the opportunity to serve alongside my wife. Many local citizens waited several hours in line, often alongside family members, simply for the opportunity to receive care. Their gratitude, trust, and resilience left a lasting impression. It was a powerful reminder that what we do extends beyond procedures. It directly influences comfort, confidence, and quality of life.
7. You participated in this mission alongside your wife, who is a general dentist—what was it like working together in this setting?
Working alongside my wife made the experience especially meaningful. We have been incredibly blessed, and we don’t take for granted the opportunity to serve others. It’s a privilege to use our skills in a way that can directly impact patients’ lives, and something we truly cherish. Although we attended dental school together and started our careers in parallel, we don’t often have the opportunity to collaborate clinically in our day-to-day lives as much anymore, so being able to serve together in this setting was unique. She focused on restorative care while I provided endodontic treatment, and we were able to see firsthand how our roles complemented one another. It added another layer of fulfillment to the trip, both professionally and personally.
8. You also got to work alongside Dr. Justman (mentor). What was a lesson learned from Dr. Justman that you can share with us?
Let me just say, Dr. Justman is a true gem to the profession, and I was happy to be paired up with him. One of the most valuable lessons I took from Dr. Justman was the importance of clarity and composure, particularly in less-than-ideal conditions. He consistently approached the day with focused attention and our cases with emphasizing efficiency and sound decision-making. Dr. Justman was funny, kept the environment light, and ran our radiograph system and headlamps flawlessly. He also gave me and my wife some really great career and life tips. He was great in navigating the high-volume, resource-limited environment with consistency reinforced that excellent outcomes are driven by discipline and judgment, not just technology.
9. What lasting impact do you hope this type of outreach work has—both for the patients served and for the providers involved?
For patients, I hope this type of outreach expands their sense of what is possible, preserving teeth is an option and their oral health is worth investing in. For providers, experiences like this offer perspective. They highlight the reality that access to care is not universal and encourage us to think more broadly about our role in addressing that gap. Ultimately, I hope this work contributes to a continued commitment, both locally and globally, to improving access to care, because the need is significant and the impact is lasting. I see it as a powerful example of stewardship to prioritize access to care and that the AAE Foundation continues to lead with purpose and intention in this area.





Dr. Jessica Hwang is a PGY2 Resident at UCLA Endodontics and a member of the AAE’s Resident and New Practitioner Committee.
Congratulations to Michigan and its fans on winning the 2026 Men’s NCAA National Championship! Michigan secured the title with a 69–63 win over UConn, capping off an impressive tournament run.
Each year, AAE’s RNPC hosts MTA March Madness alongside the NCAA Tournament to engage resident members in a fun mid-year activity ahead of APICES season. Residents submit brackets predicting the tournament champion for a chance to win a Visa gift card. First launched in 2022, this resident-only competition has proven to strengthen engagement through friendly competition. This year, 131 residents participated—marking our highest level of engagement to date!
Congratulations to the winners of the 2026 MTA March Madness:
1st Place ($400 Gift Card): Dr. Jordan Langston — Naval Postgraduate Dental School
2nd Place ($200 Gift Card): Dr. Kenny Cho — University of Washington
3rd Place ($100 Gift Card): Dr. Andrew Robbins — University of Tennessee
By Dr. Keriann Jimenez
da Silva-Filho JE, Rodrigues-Lima AC, et al. Cemental Tear: Systematic Review and Thematic Analysis of Clinical and Imaging Features with a Proposed Diagnostic Framework. J Endod, 2026;52,202-211.
Methods: This systematic review and thematic analysis looked at clinical characteristics, diagnosis, management, and outcomes of cemental tears (CT). Electronic databases were searched for published human case reports and case series describing CT. Included studies reported clinical and/or radiographic findings with confirmed diagnoses. Information collected included patient demographics, tooth type, signs and symptoms, imaging characteristics, diagnostic methods, treatment approaches, and clinical outcomes.
Results: Cemental tear was identified as a rare and underdiagnosed condition, most commonly occurring in older patients and affecting posterior teeth. Clinical presentation can mimic vertical root fracture or localized periodontal disease i.e. isolated deep probing depths, sinus tracts, and localized bone loss. Radiographic features were variable and often nonspecific, occasionally showing radiopaque fragments or J-shaped radiolucencies. Definitive diagnosis was frequently delayed and often required surgical exploration for direct visualization of detached cementum. The most common treatment was surgical removal of the cemental fragment with periodontal debridement. Outcomes were generally favorable when the fragment was removed and defects were appropriately managed; however, delayed diagnosis and extensive periodontal destruction were associated with poorer prognosis.
Conclusions: Cemental tear is an underrecognized condition that can mimic vertical root fracture and periodontal lesions, contributing to frequent misdiagnosis. Because clinical and radiographic findings are often inconclusive, surgical exploration may be necessary for definitive diagnosis. Early recognition and removal of the cemental fragment are critical for optimal healing and tooth preservation. Clinicians should include cemental tear in the differential diagnosis of isolated periodontal defects or VRF-like presentations, particularly in older patients.
Methods: Clinical case report/series evaluating the occurrence and management of a separated endodontic instrument that migrated beyond the root canal system. Clinical and radiographic examinations, including CBCT, were used to assess the position of the fragment and its relationship to adjacent anatomical structures, particularly the mandibular canal. Treatment planning focused on diagnosis, risk assessment for neurologic involvement, and selection of an appropriate management strategy. The patient had NSRCT #31 in private practice where an instrument was separated seven years prior and was referred to an endodontic program at a University Hospital (Kanagawa Hospital, Japan) and found that the instrument had migrated out of the tooth and into the mandibular canal. The patient’s medical history was significant for chronic myeloid leukemia. The Semmes-Weinstein monofilament test was used for quantitative sensory.
Results: A separated endodontic instrument in a mandibular molar can migrate into the mandibular canal, posing a risk for neurologic complications. Radiographic evaluation revealed displacement of the fragment beyond the root apex into close proximity or direct involvement with the inferior alveolar nerve. There was a minimal difference in tactile sensitivity according to the Semmes-Weinstein monofilament testing (0.1 g on the affected side vs 0.55 g on the contralateral side), and there were no clinically significant neurological symptoms that developed as a result. Management strategies depend on the location of the fragment and symptoms e.g. monitoring, surgical intervention. Follow-up radiography at 8 years showed continued migration toward the inferior mandibular border without symptom development. This case emphasizes the importance of careful assessment prior to intervention due to the potential for nerve injury.
Conclusion: Separated endodontic instruments may migrate into the mandibular canal and create a risk for neurologic complications. Accurate diagnosis and appropriate imaging is critical for identifying the position of the fragment and guiding treatment decisions. Clinicians should exercise caution and consider proximity to vital structures when determining whether to intervene or monitor. Early recognition and appropriate referral or surgical planning is essential to minimize the risk of permanent nerve injury.
Methods: Clinical study to quantify and compare the density and phenotype of sensory innervation in symptomatic vs asymptomatic apical periodontitis (AP) lesions, and to evaluate the expression of nociceptive voltage-gated Na channels in relation to clinical symptoms. Two soft tissue biopsy samples were collected during endo surgery from patients w/ persistent AP,10 of which were symptomatic and 10 asymptomatic, for a total of 40 biopsy samples. Protein extraction and ELISA were used to quantify β-tubulin III (a neural axon marker), Nav1.8, and Nav1.9, normalized to total protein content. Immunohistochemistry and confocal microscopy were performed to qualitatively assess nerve fiber density and co-localization of nociceptive markers.
Results: Symptomatic AP lesions demonstrated a 6x increase in innervation density compared with asymptomatic lesions. Expression of the nociceptive Na+ channels Nav1.8 and Nav1.9 was significantly higher in symptomatic cases. Immunohistochemical analysis revealed dense networks of nerve fibers in symptomatic lesions, predominantly composed of nociceptive fibers expressing Nav1.8, whereas asymptomatic lesions exhibited sparse innervation. These findings were independent of histopathologic lesion type.
Conclusion: Symptomatic AP is characterized by significantly increased sensory innervation and upregulation of nociceptive Na channels Nav1.8 and Nav1.9. These neural changes likely contribute to pain perception and may explain difficulties in achieving profound LA in symptomatic AP cases.
Dr. Keriann Jimenez is a member of the AAE’s Resident and New Practitioner Committee.
By Derek T. Peek, DDS, MS
I grew up around two things: teeth and airplanes.
My grandfather was a pilot who served as the Engineering Officer for the 412th Bomb Squadron of the 95th Bomb Group stationed in England during World War II, ultimately finishing the war as a captain and earning both a Bronze Star and the World War II Victory Medal. Aviation, to him, meant discipline under pressure — the understanding that every aircraft, every system, and every decision had to be right, because lives depended on it.
My father practiced endodontics for 45 years, and from him I learned that excellence in our specialty is not accidental. It is deliberate. It is systematic. It begins long before a handpiece ever touches enamel.
For most of my life, those two worlds ran parallel. Only recently did I realize how much they have in common.
When I began flight training, I expected to learn aerodynamics and airspace regulations. What I did not expect was how profoundly aviation would reshape the way I practice endodontics.
Diagnose First. Treat Second.
In aviation, you do not simply “go flying.”
You assess weather at departure and destination. You evaluate aircraft performance, fuel reserves, alternates, crosswinds, airspace, and your own readiness. Only after structured risk assessment do you make the go/no-go decision.
Endodontics should be no different.
We diagnose first. We gather clinical findings, pulpal testing, restorative assessment, periodontal evaluation, and increasingly, CBCT imaging. Only then do we determine whether treatment is appropriate.
In aviation, weather determines whether a flight should proceed. In endodontics, biology and restorability serve the same role.
Just because you technically can perform a procedure does not mean you should. Aeronautical Decision Making teaches pilots to identify hazards, assess risk, and mitigate threats before takeoff. In our operatories, that translates to thoughtful case selection — evaluating structural prognosis, medical stability, and long-term success before initiating treatment.
This diagnostic discipline is something the American Association of Endodontists has long emphasized through education and evidence-based care. As specialists, we are trained to pause, assess, and think critically before intervening. Aviation reinforced for me that this mindset is foundational to safety.
Declining treatment when risk outweighs benefit is not weakness — it is professionalism.
Layered Protection: The Swiss Cheese Model
In aviation safety, there is a concept known as the Swiss Cheese Model. It reminds us that accidents rarely result from a single catastrophic mistake. More often, they occur when multiple layers of defense — each with small imperfections — briefly align.
Endodontics is not so different.
Our defensive layers include diagnosis, CBCT imaging, magnification, rubber dam isolation, irrigation protocols, medical history review, blood pressure monitoring, documentation, and follow-up. A missed radiographic cue alone may not cause failure. Time pressure alone may not cause harm. But when small vulnerabilities align, outcomes can suffer.
The answer is not perfection. It is layered protection.
The culture of our specialty — reinforced through AAE meetings, continuing education, mentorship, and peer collaboration — strengthens these layers. Aviation simply gave me language to describe what our specialty already strives to do: build systems that reduce preventable risk.
One company that exemplifies this philosophy is Cirrus Aircraft, whose emphasis on training, standardization, and safety innovation — including the Cirrus Airframe Parachute System (CAPS) — has helped lead a transformation in safety culture across modern general aviation.
Checklists, Currency, and Preparedness
Pilots must maintain currency. To carry passengers, we must complete three takeoffs and three landings every 90 days. Emergency procedures are reviewed regularly, and checklists are non-negotiable — not because pilots lack skill, but because systems protect against human limitation.
That mindset has influenced how I run my practice.
We revisited our emergency protocols and invested in improved monitoring equipment, including a high-quality blood pressure cuff. On more than one occasion, it has revealed uncontrolled hypertension in patients who were unaware of their condition and allowed referral before treatment began. That layer of protection prevented a potential medical emergency.
We also rehearse critical scenarios — syncope, allergic reactions, hypertensive urgency — because readiness matters. Just as landings must be practiced to maintain proficiency, emergency response in a dental office must remain current.
Professionalism is not merely technical competence. It is preparedness.
CBCT as the Preflight Briefing
Before every flight, I review departure weather, en route conditions, and destination forecasts. I consider worst-case scenarios and alternates. The goal is not to eliminate risk — that is impossible — but to anticipate it.
CBCT imaging has become the endodontic equivalent of the comprehensive weather briefing.
Before rubber dam placement and access, I want to understand canal anatomy, curvature, root thickness, sinus proximity, resorptive defects, and potential perforation risk. I mentally walk through the case before I ever pick up a handpiece.
In aviation, we “chair-fly” procedures before executing them. In endodontics, CBCT allows us to “pre-treat” the case cognitively. When surprises are minimized, stress is reduced — and outcomes improve.
The mission in aviation is safe arrival. The mission in endodontics is predictable healing. Both require thoughtful planning before action.
Learning to fly as an adult has been humbling. It reminded me what it feels like to be a beginner again — to study regulations, practice maneuvers repeatedly, and submit to evaluation.
My grandfather’s B-17s required precision engineering and teamwork. My father’s decades in endodontics required the same quiet discipline. Through the education and community fostered by the American Association of Endodontists, our specialty continues that tradition of deliberate, systems-based care.
And nowhere is that more evident than in the residents preparing to lead our specialty.
Pilots are taught a simple but powerful principle: “Aviate, Navigate, Communicate.” In moments of stress, priorities matter. First, keep the aircraft flying. Second, understand where you are and where you are going. Only then communicate.
Endodontics follows a similar hierarchy. First, establish control of the clinical environment — diagnosis, isolation, visualization, and access. Next, understand the anatomy and chart the path forward. Only then do we communicate clearly with patients and colleagues about prognosis and outcomes.
Flying also offers another lesson that dentistry may be able to learn from: structured progression through training and demonstrated competency. Student pilots do not simply climb into increasingly complex aircraft or situations without preparation. Before flying certain airplanes, flying solo, or flying cross-country, pilots must receive specific instruction and earn instructor endorsements verifying they are ready for the next level of responsibility.
Endodontic education already emphasizes strong fundamentals, but aviation’s model of incremental skill endorsement is an interesting one to consider. As our specialty continues to evolve — with advanced imaging, complex retreatments, and new technologies — there may be opportunities to think creatively about how we teach and validate competency for increasingly complex procedures.
Planes and teeth may seem worlds apart, but both demand discipline, systems thinking, mentorship, and humility.
And perhaps one day those parallels will extend even further — maybe at a continuing education fly-in event humorously titled “Rudders and Root Canals,” where we explore CBCT, clinical standards, safety systems, and mentorship — both on the ground and in the clouds.
In many ways, the principle is the same in both professions: aviate, navigate, communicate.
Because whether in the sky or in the operatory, the mission is remarkably similar: to bring people home safely —and to save as many natural teeth as are truly Worth Saving.
Dr. Peek’s grandfather, Chet Peek

Dr. Peek after he passed his check ride

Dr. Peek with his father in the office

Dr. Peek with his grandfather at fly in
Dr. Derek T. Peek, DDS, MS is a Board-certified endodontist in private practice in Cedar Rapids, Iowa, and a Diplomate of the American Board of Endodontics. He is actively involved in organized endodontics and enjoys lecturing on clinical decision-making, CBCT integration, and practice systems. Outside the operatory, Dr. Peek is a private pilot who enjoys exploring the parallels between aviation safety and endodontic practice.
The future of endodontics took center stage at the AAE26 Resident Reception, where residents from programs across the country gathered for an evening of connection, conversation, and community.
Held at the Hyatt Regency Salt Lake City, this dedicated event offered a welcoming space for the specialty’s newest members to step away from the meeting schedule and focus on building meaningful professional relationships. Throughout the hour, residents connected with peers, reconnected with colleagues from dental school, and expanded their networks in a relaxed, informal setting.
With food, drinks, and a lively atmosphere, the reception struck the perfect balance between fun and professional growth. Conversations flowed easily as attendees shared experiences, discussed career paths, and strengthened the bonds that will carry forward into their careers.
As AAE26 highlighted innovation and excellence across the specialty, the Resident Reception served as a powerful reminder that its future is in capable hands. The energy, enthusiasm, and engagement on display made this event a standout moment of the meeting—and a meaningful investment in the next generation of endodontists.