Management of Severe Curvatures and Complex Anatomy: A New Approach
By Drs. Antonis Chaniotis, Anastasia Chanioti, and Ronald Ordinola Zapata
Introduction
Successful root canal preparation begins with negotiation and establishment of a smooth radicular tunnel from the canal orifice to the physiologic terminus—the glide path (1). Although a natural glide path usually exists in most roots, its dimensions, geometry, and content often make it difficult to negotiate, particularly in canals that are abruptly curved and constricted (2).
Contemporary martensitic engine-driven nickel-titanium (NiTi) instruments are extremely flexible and capable of following established canal anatomy (3). However, their safe use generally requires a reproducible glide path at least equivalent to an ISO 10 file with a .02 taper. When the anatomy prevents a size 10 K-file from reaching the radiographic terminus, because of abruptly curved and constricted canals, the clinician is confronted with what may be defined as a challenging glide path (1). In these situations, conventional instrumentation strategies may lead to procedural errors such as ledging, transportation, or instrument separation (4).
Establishing and enlarging a glide path in complex anatomy therefore remains one of the most critical steps in endodontic treatment (Fig 1).
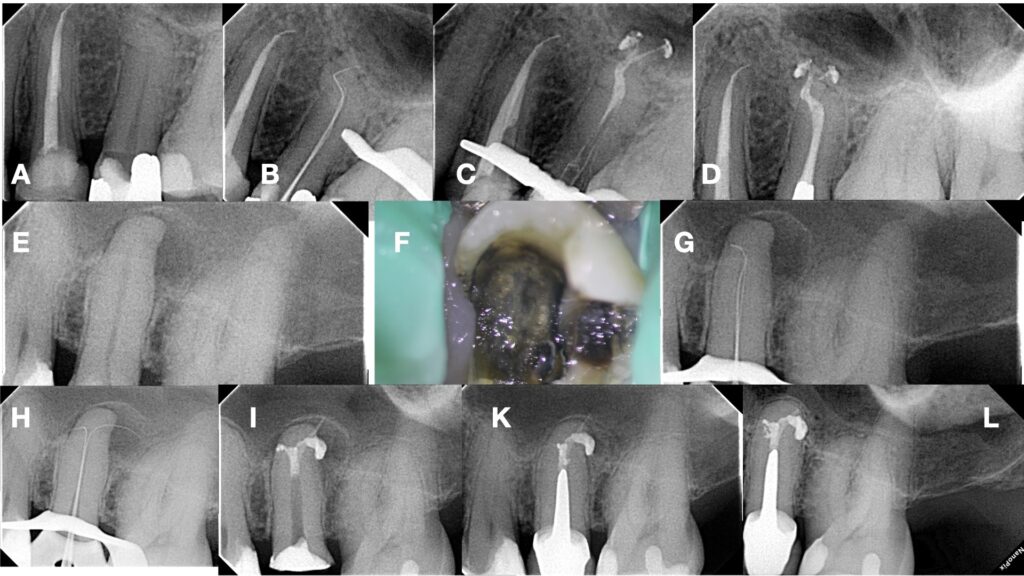
Figure 1. A-D. Challenging splitting and double curved apical glidepath negotiation in a second maxillary premolar, E-I. Challenging splitting highly curved anatomical glidepath negotiation in a second maxillary premolar, K & L. 1 year and 15 years follow up radiographs.
Challenges in Initial Canal Negotiation
Small stainless steel hand files remain the primary instruments for initial canal exploration. Their flexibility allows them to follow narrow pathways; however, they frequently lack the rigidity required to negotiate constricted or calcified canals (5). Under apically directed watch-winding motion, these instruments may buckle or distort.
Conversely, tapered hand files possess greater stiffness but are often too bulky to pass through constricted regions of the canal system. To address this limitation, several manufacturers have introduced specialized glide-pathfinding instruments (e.g., C- files, D-finders) designed to enhance penetration through calcified pathways (5). These instruments typically feature modified tip geometries, heat-treated stainless steel for increased rigidity, or carbon steel alloys that enhance cutting efficiency.
Various design modifications—including alterations in taper, cross-section, and metallurgy—have attempted to balance three critical factors: small tip size, sufficient rigidity, and resistance to deformation (6). Despite these advances, severe canal curvature combined with calcification continues to present a significant clinical challenge.
Negotiation and “Follow” Strategy
Once a canal orifice is identified, initial exploration can begin with a slightly pre-curved ISO size 10 K-file (.02 taper). The file tip is gently introduced into the orifice and allowed to passively follow the canal trajectory. Using delicate watch-winding movements with minimal apical pressure, the file is allowed to “slide” within the canal until resistance is encountered (1).
If the file reaches working length without obstruction, engine-driven instrumentation may begin. However, when the file becomes blocked short of the radiographic terminus—often at an abrupt curvature—the clinician must adopt strategies to secure the glide path (1).
When curvature prevents further negotiation, both the radius and position of the curvature must be estimated and replicated on the scouting file (Fig. 2). Pre-curving the apical portion of the file allows the instrument tip to be oriented toward the inner wall of the curvature (Fig.3). In canals with abrupt curvatures, coronal pre-flaring may be necessary to allow the pre-curved file to enter the canal.
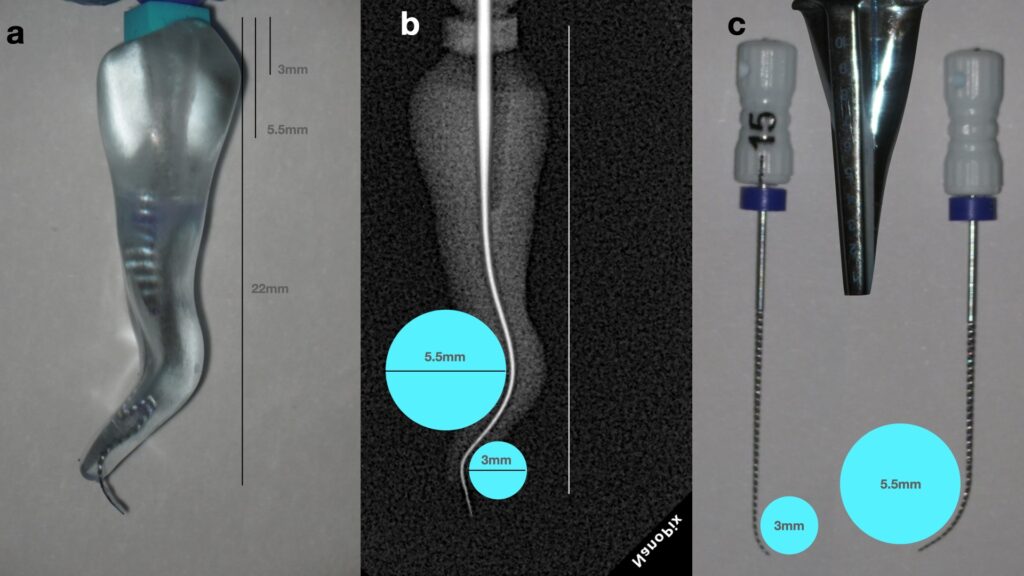
Figure 2. A. Double curved transparent 3D printed tooth for practicing and teaching challenging root canal negotiation (drsk.com, Sweden), B. Radiographic evaluation of the curvatures and measurement of the radius of the middle and apical third curvatures, C. Replication of the different radius of the curvatures in a 15 k-file by using the Endo Bender tool (Sybron endodontics)
The pre-curved file is then gently guided to the point of obstruction with watch-winding movements and no apical force. At the curvature, the instrument is rotated so that the tip faces the inner aspect of the curve, enabling it to negotiate beyond the blockage.
A notched silicone stop on the file can help control the spatial orientation of the pre-curve. In some cases, introducing a secondary apical curve in a different plane facilitates negotiation of complex three-dimensional anatomy (1).
Once the tip negotiates beyond the curvature, the envelope of motion technique can be applied. In this maneuver, the file is rotated clockwise while maintaining slight coronal resistance to prevent apical screwing-in (Fig 3). This movement selectively removes dentin from the coronal aspect of the curvature, slightly increasing the curvature radius and smoothing the pathway (7).
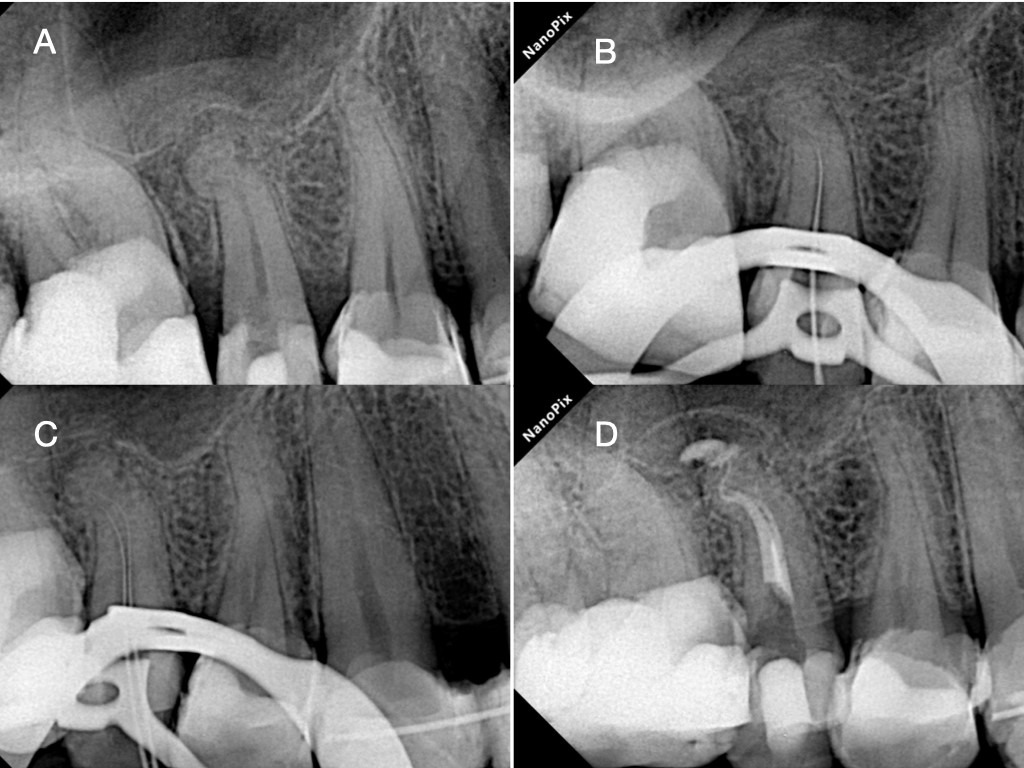
Figure 3. A. Preoperative periapical radiograph revealing apical anatomic complexity in the second maxillary premolar, B. Intraoperative Periapical Radiograph revealing the blocked glidepath in the level of the first curvature, C. Intraoperative periapical radiograph revealing the negotiation result around the first curvatures after applying the negotiation and follow strategy, D. Postoperative periapical radiograph after TCA instrumentation and obturation procedures
Gradually, the canal becomes easier to negotiate, and the file may advance to the radiographic terminus using gentle watch-winding movements. Once working length is achieved, short amplitude “smoothing” motions (<0.5 mm) help loosen the file and refine the glide path.
At this stage, when a size 10 K-file becomes extremely loose and reproducible, engine-driven NiTi instrumentation may be initiated.
Glide Path Enlargement with the Tactile Controlled Activation (TCA) Technique
In canals with severe curvature, conventional rotary instrumentation can generate significant torsional and cyclic stresses. To reduce these stresses, Tactile Controlled Activation (TCA) instrumentation was introduced (8).
TCA is defined as single-stroke activation of a stationary engine-driven file only after passive engagement within a patent canal provides tactile feedback regarding canal anatomy. The concept is based on maximizing passive engagement below the curvature before file activation, thereby minimizing torsional stress.
The technique consists of three phases: stationary, in-stroke, and out-stroke (2).
Stationary Phase
After access preparation and canal location, technical patency and a glide path to at least size 10/.02 are established. The first rotary instrument selected should have a tip size smaller than the dimensions of the patent glide path at the level of the abrupt curvature, with a taper preferably ≤4%.
The file is mounted in the endodontic motor but introduced into the canal without rotation, passively advancing until frictional resistance is encountered. In difficult access situations, the file may be inserted manually before connecting the motor intraorally.
In-Stroke Phase
Before activation, the clinician must confirm that the file tip is positioned below the first curvature, not above it. This may be verified radiographically or by precise measurement of the curvature depth.
Once the correct position is confirmed, the file is activated and passively left to advance apically until the first point of resistance is encountered beneath the curvature.
Out-Stroke Phase
When resistance is reached, the instrument is withdrawn from the canal without further apical pressure. During withdrawal, the file may be directed toward the bulkier root structure—away from the thin “danger zone”—in an anti-curvature motion.
This single in-stroke/out-stroke movement allows dentin removal while reducing the risk of torsional failure. The file transitions from maximum passive engagement (stationary) to minimal engagement during activation, reducing stress accumulation.
After removal, the file flutes are cleaned and inspected for deformation. Irrigation is performed and patency is reconfirmed. During the next stationary phase, the same instrument will typically bind slightly deeper in the canal.
The cycle is repeated in a crown-down progression until the file reaches working length with single TCA strokes. Once a file can reach working length without activation during insertion, its shaping task is considered complete. Subsequent instruments enlarge the preparation to the desired apical diameter and taper using the same controlled approach. The combination of the glidepath securing technique with the single stroke Tactile Activation Technique (TCA) will ensure the safe and uneventful instrumentation of challenging abruptly curved canal trajectories allowing the preservation of the original anatomy (Fig 4, 5).
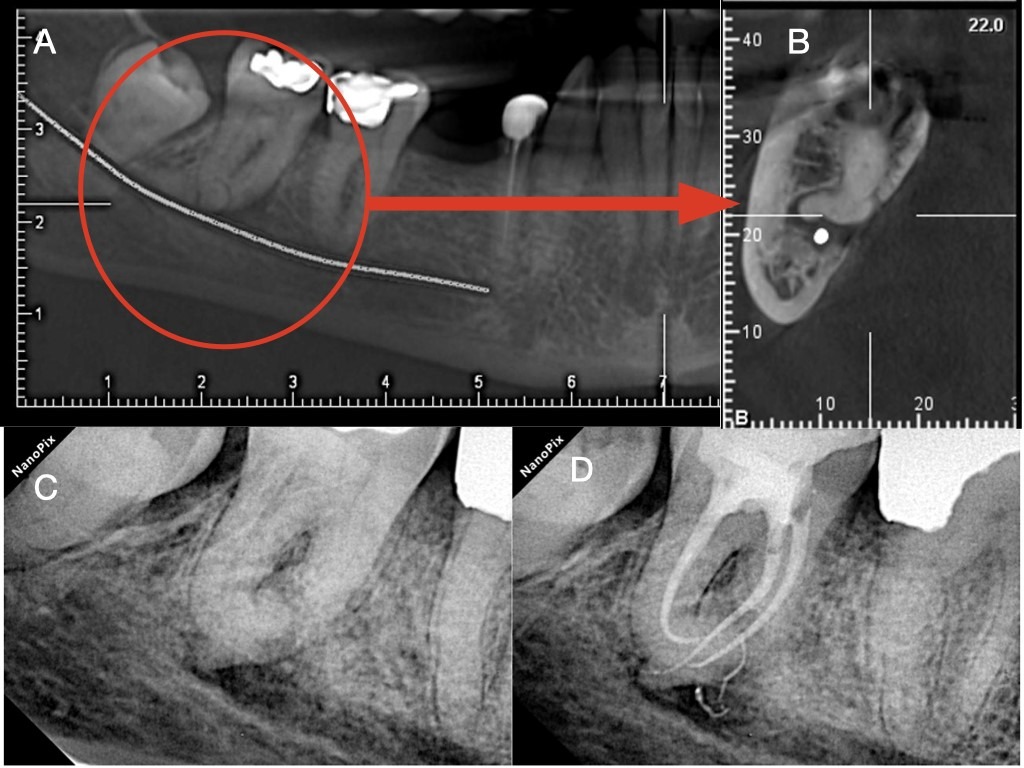
Figure 4. A. Panoramic CBCT view of a second mandibular molar with buccally oriented abrupt curvature (Bull’s eye), B. The Sagittal CBCT view revealing the parameters of the abrupt curvature (topography, length, radius and angle of curvature), C. Pre-operative 2 dimensional radiograph of the same tooth, D. Postoperative radiograph after following the glidepath negotiation and TCA instrumentation strategy.
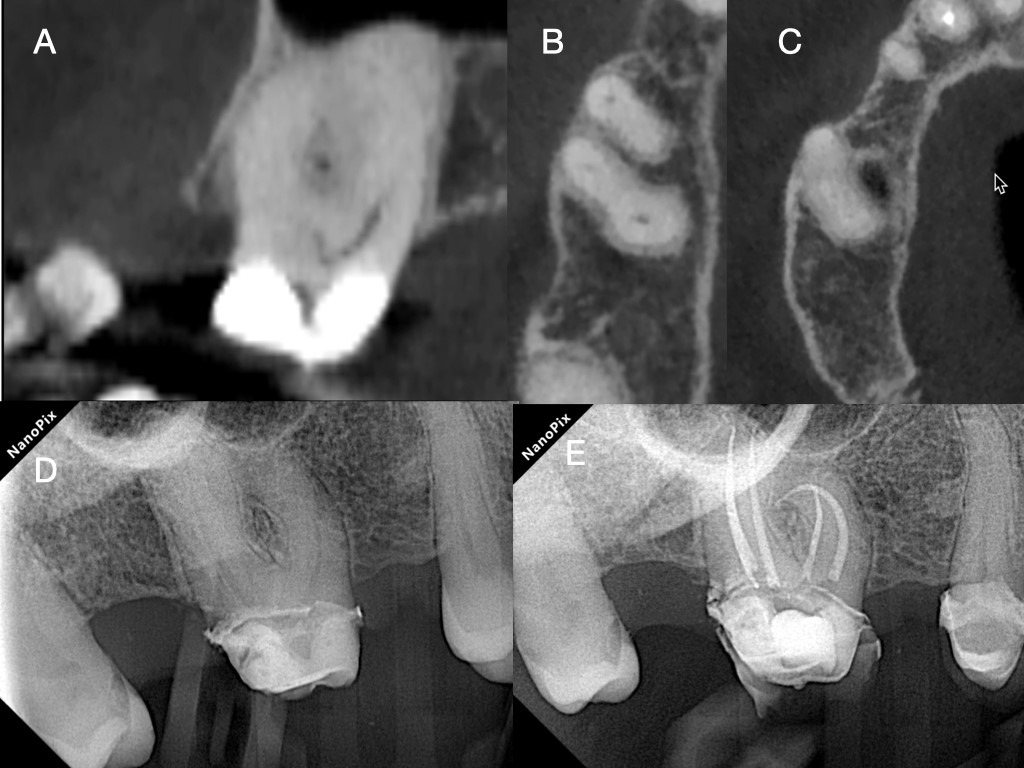
Figure 5. A. Panoramic CBCT view of a second maxillary molar with complicated highly curved apical anatomy suggesting a challenging glidepath, B &C. The axial CBCT views of the same tooth revealing fusion of the roots, C. Pre-operative 2-dimensional radiograph of the same tooth, D. Postoperative radiograph after following the glidepath negotiation and TCA instrumentation strategy.
Flexible martensitic NiTi instruments with non-cutting tips are best suited for TCA. Instruments with strong restoring forces or cutting tips may increase the risk of ledging when activated within a curvature and are contraindicated to be used with this technique (2).
Clinical Considerations
The TCA technique aims to deliver adequate apical preparation in severely curved canals while minimizing the duration of active engagement around curvatures. By emphasizing tactile feedback and controlled activation, the approach seeks to reduce torsional stress and procedural errors.
Although clinical experience suggests that the method may be particularly advantageous in complex anatomies—including constricted and abruptly curved canals—independent investigations evaluating its limits remain limited. As with all advanced instrumentation techniques, careful case selection and clinician judgment remain essential.
References
- West JD. The endodontic Glidepath: ‘‘secret to rotary safety.’’ Dent Today 2010;29: 90-93.
- Chaniotis A, Ordinola-Zapata R. Present status and future directions: Management of curved and calcified root canals. Int Endod J. 2022 May;55
- Peters OA. Current challenges and concepts in the preparation of root canal systems. J Endod. 2004.
- Bürklein S, Werneke M, Schaefer E. Impact of glide path preparation on the incidence of dentinal defects after preparation of severely curved root canals. Quintessence international 2018;49(8):607-613
- Allen, M. J., Glickman, G. N., & Griggs, J. A. (2007). Comparative analysis of endodontic pathfinders. Journal of endodontics, 33(6), 723–726.
- Cormier, C. J., von Fraunhofer, J. A., & Chamberlain, J. H. (1988). A comparison of endodontic file quality and file dimensions. Journal of endodontics, 14(3), 138–142.
- Yu DC, Tam A, Schilder H (2009). Patency and envelope of motion–two essential procedures for cleaning and shaping the root canal systems. General dentistry 57, 616–621.
- Chaniotis A, Filippatos C (2017) Root canal treatment of a dilacerated mandibular premolar using a novel instrumentation approach. A case report. International Endodontic Journal 50, 202–211
Dr. Antonis Chaniotis is in private practice and a clinical fellow teacher, National and Kapodistrian University of Athens, Dental School, Department of Endodontics, and Chair, Clinical Committee of the European Society of Endodontology. Orcid: https://orcid.org/0000-0003-2844-5338
Dr. Anastasia Chanioti is a dentist affiliated with the National and Kapodistrian University of Athens, Dental School, Department of Endodontics. Orcid: https://orcid.org/0000-0003-3535-1655
Dr. Ronald Ordinola Zapata is from the Endodontic Division, Department of Restorative Sciences. University of Minnesota School of Dentistry, Minn. Orcid: https://orcid.org/0000-0001-9738-0828
The authors can be reached at chaniotisantonis@gmail.com.
Disclaimer
The views and opinions expressed by authors are solely those of the authors and do not necessarily reflect the official policy or position of the American Association of Endodontists (AAE). Publication of these views does not imply endorsement by the AAE.