Rethinking Decompression of Large Cystic Periapical Lesions in the New Era

By Feng-Ming Wang, DDS, PhD
Deroofing of the jaw cyst (the original strategy of decompression) was first suggested by Partsch in the German literature in 1892 (1). In 1964, Patterson reported a successful decompression by using a polyethylene tube and stint for drainage on a large periapical lesion associated with the left central and lateral incisors on a 26-year-old patient (2). This was right after endodontics being formally approved as the 8th dental specialty by the American Dental Association House of Delegates in 1963. After many years, decompression appears to be an overlooked alternative approach for managing large cystic periapical lesions (3).
Nonsurgical root canal treatment on anterior teeth has a success rate of 74% in a 2004 study (4) and 59% in a 2024 study (5). In the latter study, if the outcome was evaluated by Cone-Beam Computed Tomography (CBCT), the success rate dropped to 20% (5). Endodontists have seen that despite the advancement of the knowledge of endodontics and modern technology, there are lesions that do not heal after nonsurgical root canal treatments. Often, periapical surgery is chosen to address the situation of non-healing periapical lesions following nonsurgical treatments and retreatments. But challenges exist due to the pitfalls of periapical surgery. Most common ones include jeopardizing the osseous support of adjacent teeth, damage to the blood vessels, nerves of adjacent teeth, and anatomic structures like canalis sinuosus in the anterior maxilla (6), and occurrence of a surgical defect. Sometimes patients cannot tolerate the procedure well because of their age and/or health conditions. Thus, it is important to know that decompression can be a great substitute of periapical surgery when such dilemma presents.
Understanding the pathogenesis of periapical cyst would help us understand the decompression technique so that we could use it comfortably to manage large cystic periapical lesions. There are at least three popular theories regarding the formation of periapical cyst. First, in the nutritional deficiency theory, as islands of epithelium expand, more central epithelial cells are distanced from their nutritional supply and undergo necrosis. A cystic cavity results in the center of the cell mass as liquefaction necrosis occurs (7). Second, in the immunological reaction theory, inflammatory mediators from the immune reactions stimulate epithelial cell rests of Malassez (ERM) to proliferate, resulting in cystic lined lumen formation (8). Third, in the abscess theory, cavity comes into existence and starts to be lined by the epithelium from the proliferating ERM led by inflammatory mediators; cavity enlarges due to osmotic pressure with the lack of lymphatic circulation and pressure-induced resorption of the surrounding bone (9-11). The degenerative characteristics of epithelial linings continues enhancing osmolality of the cyst contents till pressure is relieved. Although the pathogenesis of the periapical cyst remains to be elucidated, clinical cases evidenced that irrigation after aspiration with or sometimes even without long-term decompression can achieve optimal outcomes. The possible explanation of treatment efficacy could include the following: 1) diminishment of osmotic pressure after the integrity of the lesion wall is disrupted; 2) reduction the impact of inflammatory mediators on epithelial cells after the lesion content is aspirated and rinsed; 3) introduction of bleeding and blot clotting followed by new blood vessel formation and then tissue regeneration, especially bone formation as a wound healing process. Further, it has been proposed that the epithelial cells would experience programmed cell death (apoptosis) in response to the lack of the inflammatory mediators (12).
According to Glossary of Endodontic Terms, decompression aims to reduce the size of a large cystic periapical lesion using two primary techniques: 1) the surgical incision through a wall and insertion of a drain; 2) the penetration of the cyst in two locations with two large gauge needles and flushing with sterile saline (13). There are several types of drain technique described in the literature (3). Manjarrés and colleagues developed a 3D-printed educational model for decompression and nicely showcased its application clinically (14). The author of this Communiqué article has recently successfully used Penrose drain in treating several cases of large cystic periapical lesion. One of the author’s publications showed that decompression using the Penrose drain significantly induced bone regeneration and reduced lesion size before periapical surgery was performed later (15). Penrose drain was named after Charles B. Penrose (1862-1925) physician specializing in gynecology. Penrose drain is soft, radiopaque, and inert, with minimal foreign body reaction. It provides patients with comfort and can be located radiographically. The length of drainage in literature ranged from 2 days (16) to 5 years (17). The author found that 4-week period had worked well in all their cases. Hoen and colleagues reported that aspiration followed by irrigation without further placement of drain achieved great results as well (18). As shown in Figure 1, the healing of large cystic lesion associated with teeth #7 and #8 in an 85-year-old female was demonstrated by CBCT imaging following aspiration and irrigation only. Nevertheless, the author recommends that clinicians should determine the length of drainage case by case. Of note, it appears unnecessary or sometimes impractical for patients to perform self-irrigation of the lesion with saline or some type of antibacterial agent.
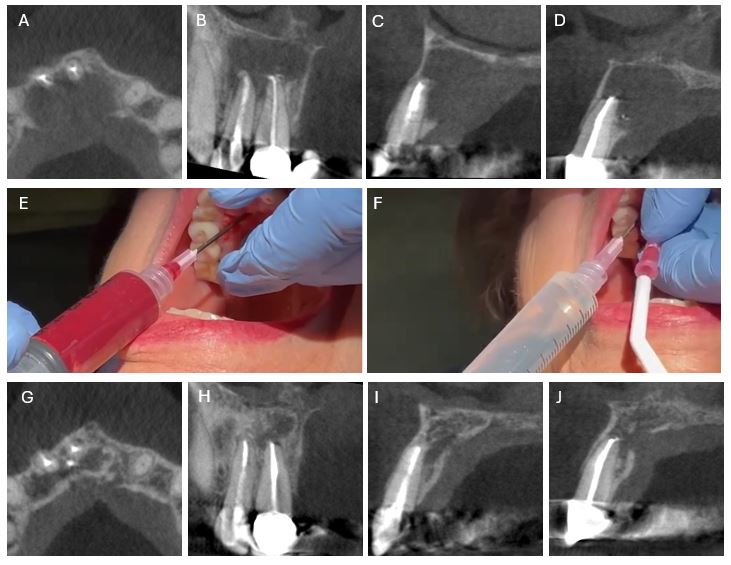
Figure 1 – Management of large periapical lesion by decompression. An 85-year-old female presented with pain and swelling in the anterior palate. A-D) Preoperative limited field of view CBCT scan. A) Axial view. B) Coronal view of teeth #7 and #8. C) Sagittal view of tooth #7. D) Sagittal view of tooth #8. E) Decompression by aspiration using an 18-gauge needle. F) Irrigation of the lesion with saline using 2 needles. G-J) Three-year follow-up CBCT scan. G) Axial view. H) Coronal view of teeth #7 and #8. I) Sagittal view of tooth #7. J) Sagittal view of tooth #8. (This work was done by Dr. Wang together with his former resident Dr. Ghazaleh Rezaei, who currently practices at Las Vegas Endodontics. CBCT scans were kindly provided by Dr. Matthew Massey at Heart of Texas Endodontics.)
It is worth mentioning that a large periapical lesion does not automatically mean a cyst. The proportion of periapical cysts increases when lesion increases in size (19). But some very large lesions have been confirmed to be granulomas through biopsy. Provisionally, a periapical lesion could be diagnosed as a cystic lesion when it involved one nonvital tooth and the straw-colored fluid was aspirated from the lesion (20).
In general, decompression may be considered in cases involving nonvital teeth or teeth associated with a large radiolucent lesion (more than 200 mm2) when needle aspiration demonstrates a straw-colored fluid or copious drainage from the canal during root canal therapy. The cystic cavity should allow free placement of a tube or drain within the lesion. Decompression should not be recommended for lesions with a chronic sinus tract. If upon attempting aspiration, the clinician is unable to remove fluid from the bony cavity, this would indicate the presence of granulomatous lesion which is unsuitable for decompression. Like any other surgical procedures, it is always important to review medical and dental history and evaluate risks thoroughly prior to decompression of large periapical lesions.
In summary, decompression is a preservative and minimally invasive approach to manage large cystic periapical lesions. Endodontists should be aware of this treatment option and may offer it to understanding and motivated patients before more aggressive surgical procedures are selected.
Dr. Feng-Ming Wang is a Clinical Associate Professor of Endodontics in Texas A&M University College of Dentistry and maintains a private practice at Precision Endodontics in Plano, Texas. The author would like to thank Dr. James L. Gutmann for kindly reviewing the article.
Reference
- Partsch C. Über kiefercysten. Deutsche Monatsschrift Fur Zahnheilkunde. 1892(10):271-304.
- Patterson SS. Endodontic therapy: Use of a polyethylene tube and stint for drainage. J Am Dent Assoc 1964;69(6):710-714.
- Gutmann J, Ferreyra S. Alternative and contemporary management of large periradicular lesions. ENDO (Endodontic Practice Today) 2010;4(2):127-144.
- Caliskan MK. Prognosis of large cyst-like periapical lesions following nonsurgical root canal treatment: a clinical review. Int Endod J 2004;37(6):408-416.
- Artaza L, Campello AF, Soimu G, Alves FRF, Rocas IN, Siqueira JF, Jr. Outcome of Nonsurgical Root Canal Treatment of Teeth With Large Apical Periodontitis Lesions: A Retrospective Study. J Endod 2024;50(10):1403-1411.
- Veronezzi MC, Pinheiro IHS, Tolentino ES, Camarini C, Takeshita WM, Iwaki LCV, et al. Anatomical variations in the maxillary anterior region: a cone beam computed tomographic study of the canalis sinuosus and its accessory canals. Gen Dent 2023;71(4):16-22.
- Ten Cate AR. The epithelial cell rests of Malassez and the genesis of the dental cyst. Oral Surg Oral Med Oral Pathol 1972;34(6):956-964.
- Torabinejad M. The role of immunological reactions in apical cyst formation and the fate of epithelial cells after root canal therapy: a theory. Int J Oral Surg 1983;12(1):14-22.
- Toller PA. Newer concepts of odontogenic cysts. Int J Oral Surg 1972;1(1):3-16.
- Valderhaug J. A histologic study of experimentally induced periapical inflammation in primary teeth in monkeys. Int J Oral Surg 1974;3(3):111-123.
- Nair PN, Sundqvist G, Sjogren U. Experimental evidence supports the abscess theory of development of radicular cysts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106(2):294-303.
- Lin LM, Huang GT, Rosenberg PA. Proliferation of epithelial cell rests, formation of apical cysts, and regression of apical cysts after periapical wound healing. J Endod 2007;33(8):908-916.
- American Association of Endodontists. (2020). Decompression. In Glossary of Endodontic Terms (10th ed., p. 14).
- Manjarrés V, Bonilla C, Guerrero M, Gutmann JL. A 3D-printed educational model for decompression and case report. ENDO (Endodontic Practice Today) 2020;14(1):71-78.
- Wang FM, Liang H, Glickman GN, Gutmann JL. Use of a penrose drain for decompression of a large periapical lesion: A case report with 4.5-year follow-up. J Endod 2024;50(10):1521-1526.
- Loushine RJ, Weller RN, Bellizzi R, Kulild JC. A 2-day decompression: a case report of a maxillary first molar. J Endod 1991;17(2):85-87.
- Rees JS. Conservative management of a large maxillary cyst. Int Endod J 1997;30(1):64-67.
- Hoen MM, LaBounty GL, Strittmatter EJ. Conservative treatment of persistent periradicular lesions using aspiration and irrigation. J Endod 1990;16(4):182-186.
- Natkin E, Oswald RJ, Carnes LI. The relationship of lesion size to diagnosis, incidence, and treatment of periapical cysts and granulomas. Oral Surg Oral Med Oral Pathol 1984;57(1):82-94.
- Eversole RL. Clinical outline of Oral pathology: diagnosis and treatment, 2nd edition. Philadelphia, PA: Lea & Febiger; 1984.
Disclaimer
The views and opinions expressed by authors are solely those of the authors and do not necessarily reflect the official policy or position of the American Association of Endodontists (AAE). Publication of these views does not imply endorsement by the AAE.