The Dynamics of Periapical Lesions in Endodontically Treated Teeth: Rationale for a Clinical Intervention

By Drs. Tomer Goldberger, Eyal Rosen and Igor Tsesis
Introduction
In various cross-sectional studies a high prevalence of apical periodontitis (AP) in endodontically treated teeth has been reported ranging from 40%–61% (1–3). Bacteria persisting in the root canal system is generally the main reason for the persistence of AP following endodontic treatment (4–9).
Management of the teeth with persistent AP may include nonsurgical endodontic retreatment, surgical endodontic treatment, or tooth extraction (10-11). However, in certain cases it may be considered leaving the tooth without intervention and adopt a long-term follow-up protocol (12). In medicine this approach is defined as a “watchful waiting”, that means closely watching a patient’s condition but not giving treatment unless symptoms appear or change (13). In case of AP, this approach may be considered due to the slowly progress of the diseases and in cases when the risks of treatment are greater than the possible benefits. What may be the consequences of treating or not treating an existing apical pathology is a crucial question, which constitutes the core of the clinical decision-making process endodontics (14).
The long-term dynamics of periapical lesions in endodontically treated teeth and possible influencing factors are not fully elucidated, thus presenting a real clinical dilemma regarding the need for an intervention.
Quality of Coronal Restoration
It is commonly believed that the outcome of root canal treatment is mostly associated with the technical quality of the root filling. Extra attention has been paid to coronal leakage as a potential cause of endodontic failure (15-16). In a study of 1010 endodontically treated teeth, Ray and Trope (17) found that the quality of the coronal restoration had a greater impact on the periradicular status than the quality of the endodontic treatment. Although some studies showed that well-prepared and filled root canals can resist bacterial penetration even without intact coronal restoration (18), other studies stressed the importance of adequate coronal restoration for periapical healing (17, 19).
Quality of Root Canal Filling
The quality of root canal filling is associated with the adequate treatment of roots. It is usually evaluated radiographically and defined as adequate in case all canals were obturated, no voids were present, and the root canal filling ended between 0 and 2 mm short of the radiographic apex. (20) The mail goal of the root canal filling is to establish a bacteria tight seal of the root canal so that oral bacteria cannot reach the periapical tissues and cause disease. Tronstad el al (17) found that if the root canal was not properly obturated, the quality of the coronal restoration had no bearing on the outcome of the endodontic treatment.
Over the years, numerous cross-sectional studies were followed in many other countries which evaluated the influence of the quality of root canal fillings and coronal restorations on the periradicular status of root canal–treated teeth. Those studies had various results; most of them concluded that the periradicular status depended equally on the quality of the root canal filling and the coronal restoration. (21-23)
The Dynamics of Periapical Lesions in Endodontically Treated Teeth That Are Left without Intervention
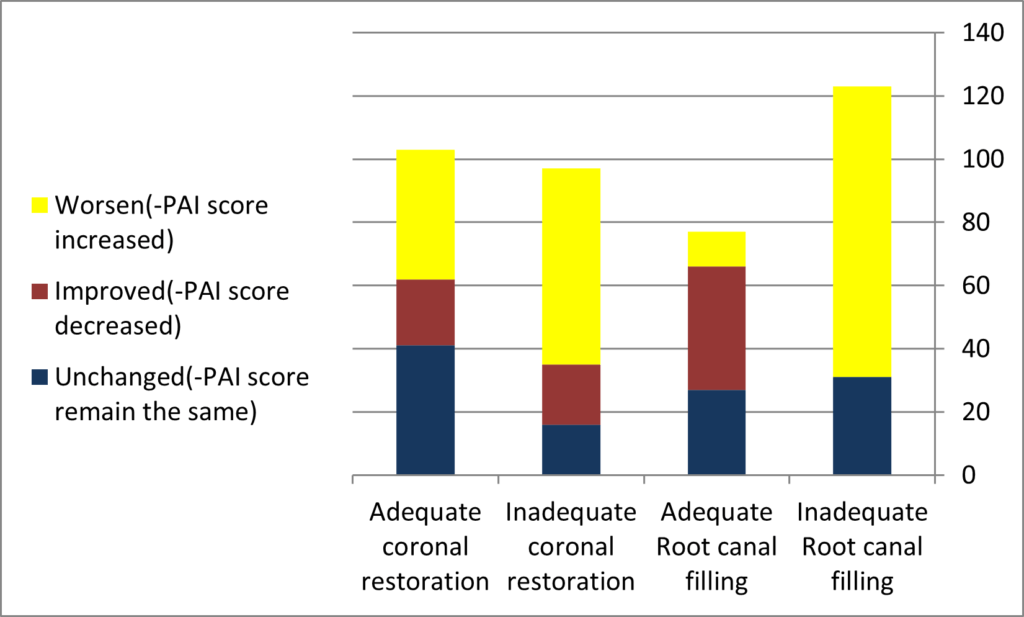
In a retrospective cohort study (24) consisted of 74 patients with a total of 200 endodontically treated coronally restored teeth having periapical lesions. The dynamics of the included periapical lesions was evaluated based on the periapical index (PAI) score changes between 2 consecutive periapical surveys of at least a 4-year interval. The influence of various factors on lesion dynamics was statistically evaluated. Fifty-seven (28.5%) lesions remained unchanged, 103 (51.5%) lesions worsened (PAI score increased), and 40 (20%) lesions improved (PAI score decreased). Poor root canal filling and poor restoration were the only factors found to adversely affect the long-term dynamics of the periapical lesions (P < .05).
Figure 1. Periapical Index (PAI) Change Between the Two Consecutive Status Surveys
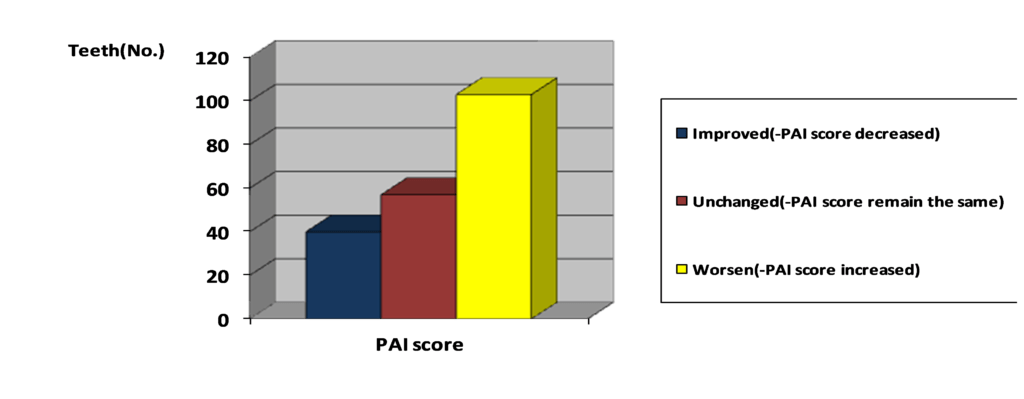
Figure 2: PAI Change in Relation to Root Canal Filling Quality and to Coronal Restoration Quality
Take-Home Message
Poor root canal filling and poor restoration may adversely affect the long-term dynamics of periapical lesions that are left without intervention in endodontically treated teeth. Therefore, in cases of poor root canal filling or poor restoration, further intervention may be indicated. However, in cases when the root canal treatment and the coronal restoration are considered adequate, the teeth with suspected AP may be left without intervention and the “watchful waiting” approach may be adopted.
References:
- 1. De Moor RJ, Hommez GM, De Boever JG, et al. Periapical health related to the quality of root canal treatment in a Belgian population. Int Endod J 2000;33:113–20.
- 2. Georgopoulou MK, Spanaki-Voreadi AP, Pantazis N, et al. Frequency and distribution of root filled teeth and apical periodontitis in a Greek population. Int Endod J 2005;38:105–11.
- 3. Kabak Y, Abbott PV. Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. Int Endod J 2005;38:238–45.
- 4. Bystrom A, Happonen RP, Sjogren U, et al. Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endod Dent Traumatol 1987;3:58–63.
- 5. Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod 1992;18:625–7.
- 6. Nair PN, Sjogren U, Krey G, et al. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. J Endod 1990;16:580–8.
- 7. Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root canal therapy: a review. Endod Dent Traumatol 1994;10:105–8.
- 8. Siqueira JF Jr. Aetiology of root canal treatment failure: why well treated teeth can fail. Int Endod J 2001;34:1–10.
- 9. SjogrenU, Figdor D, PerssonS, etal. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int Endod J 1997;30:297–306.
- Doyle SL, Hodges JS, Pesun IJ, et al. Factors affecting outcomes for single-tooth im- plants and endodontic restorations. J Endod 2007;33:399–402.
- Zitzmann NU, Krastl G, Hecker H, et al. Endodontics or implants?A review of decisive criteria and guidelines for single tooth restorations and full arch reconstructions. Int Endod J 2009;42:757–74.
- Orstavik D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int Endod J 1996;29:150–5.
- https://www.cancer.gov/publications/dictionaries/cancer-terms/def/watchful-waiting
- Kvist T, Reit C. The perceived benefit of endodontic retreatment. Int Endod J 2002; 35:359–65.
- W.P. Saunders, E.M. Saunders. Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol, 10 (1994), pp. 105-108
- M.E. Magura, A.H. Kafrawy, C.E. Brown, et al. Human saliva coronal microleakage in obturated root canals- an in vitro study. J Endod, 17 (1991), pp. 324-331
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J 1995;28: 12–8.
- Ricucci D, Bergenholtz G. Bacterial status in root-filled teeth exposed to the oral environment by loss of restoration and fracture or caries—a histobacteriological study of treated cases. Int Endod J 2003;36:787–802.
- Tronstad L, Asbjornsen K, Doving L, et al. Influence of coronal restorations on the periapical health of endodontically treated teeth. Endod Dent Traumatol 2000;16: 218–21.
- ESE. Quality guidelines for endodontic treatment: consensus report of the EuropeanSociety of Endodontology. Int Endod J 2006;39:921–30.
- Dugas NN, Lawrence HP, Teplitsky PE, et al. Periapical health and treatment quality assessment of root-filled teeth in two Canadian populations. Int Endod J 2003;36: 181–92.
- Sidaravicius B, Aleksejuniene J, Eriksen HM. Endodontic treatment and prevalence of apical periodontitis in an adult population of Vilnius, Lithuania. Endod Dent Traumatol 1999;15:210–5.
- Kirkevang LL, Orstavik D, Horsted-Bindslev P, et al. Periapical status and quality of root fillings and coronal restorations in a Danish population. Int Endod J 2000;33: 509–15.
- Tsesis I, Goldberger T, Taschieri S, Seifan M, Tamse A, Rosen E. The dynamics of periapical lesions in endodontically treated teeth that are left without intervention: a longitudinal study. J Endod. 2013 Dec;39(12):1510-5.
Drs. Goldberger, Rosen and Tsesis are from the Department of Endodontics, Maurice and Gabriela Goldschleger School of Dental Medicine, Sackler Faculty of Medicine, Tel Aviv University, Israel. Dr. Rosen is also of the Center for Nanoscience and Nanotechnology, Tel Aviv University, Israel.