Update on Irrigation Disinfection
 By Bettina R. Basrani D.D.S., M.S.D., Ph.D.; and Gevik Malkhassian, D.D.S., M.SC., FRCD(C)
By Bettina R. Basrani D.D.S., M.S.D., Ph.D.; and Gevik Malkhassian, D.D.S., M.SC., FRCD(C)
Root canal treatment aims to prevent or cure apical periodontitis, and this aim is achieved by eliminating microorganisms capable of causing an intraradicular or extraradicular infection. It is well documented that mechanical instrumentation and strong antibacterial irrigation followed by well-sealed obturation of the root canal system can significantly reduce the bacterial load and create an environment conducive to healing.
During endodontic disinfection, the clinician faces many limiting factors: such as complex root canal anatomy, untouched dentin walls left during mechanical instrumentation, and bacterial load in forms of biofilm attached to dentin walls and in the isthmus.
Many irrigating solutions and delivery systems were proposed to overcome some of these limitations. Sodium hypochlorite (NaOCl), back in 1936, was recommended by Walker to irrigate the root canals. In 1943, Grossman recommended the use of NaOCl and hydrogen peroxide. Later in 1957, Nygaard-Ostby introduced the ethylenediaminetetraacetic acid (EDTA) solution for root canal irrigation. Nowadays, there is a whole variety of irrigating solutions tested for root canal disinfection. They range from very caustic single irrigants (such as NaOCl) to herbal formulations (like chamomile or green tea). (1).
Despite all the advances made in the last 80 years, many published articles worldwide have demonstrated some controversial results, which may confuse clinicians in their selection of the best irrigation regimen.
Some of the dilemmas in selecting the best irrigating protocol during endodontic treatment are as the following:
- Duration of irrigation: How much time do I need to disinfect the canal?
- Concentration of irrigating solutions: Which concentration of NaOCl should I use?
- Disinfection of apical third of the canal: How can the irrigant reach the apical portion?
- Irrigation sequence: Which sequence of irrigants should I use?
Time (Duration):
Contact time of the irrigants and medications with the contaminated dentin is essential. For the irrigant to be effective, it requires reaching and disrupting the biofilm attached to the canal walls. However, the literature has a considerable variation on this point. In some articles, hypochlorite is reported to kill the target microorganism in seconds, even at low concentrations; other publications have reported considerably longer times for killing the same species. This difference may be formed on basis that the presence of organic matter, inflammatory exudate, tissue remnants and microbial biomass, could weaken the antibacterial effect of NaOCl solution. To overcome this limitation, continuous irrigation with a fresh solution and added contact time are essential factors to increase the effectiveness of NaOCl. (2)
Interestingly, according to some recently published studies NaOCl, when left in contact with dentin for an extended period of time, may have an unfavorable effect on dentin. 5.25% sodium hypochlorite reduces the flexural strength and elastic modulus of dentin. As a result, on one hand, more exposure time of the irrigation with the canal walls is needed to eliminate biofilm; on the other hand, this increased time could be harmful to dentin. (10, 11)
Therefore, clinicians must consider all these factors when using the different irrigants in a clinical case to enhance their favorable properties while mitigating the adverse effects.
Concentration:
Sodium Hypochlorite for endodontic irrigation is being used worldwide in a different concentration ranging from 0.5 to 6%. A higher concentration of NaOCl has been found to have better antibacterial efficacy and biofilm disruption and removal (12), also better tissue dissolving properties. However, studies have shown that lower concentrations can have similar effects when used in larger volumes and more frequent intervals. Higher concentrations of NaOCl are more toxic than lower concentrations, and if accidentally extruded beyond the root canal, the tissues’ reaction could be worse than the lower concentration. Gladly, due to the confined anatomy of the root canal system, these incidents are rare. Higher concentrations have successfully been used during root canal treatment, with a low incidence of mishaps. (2)
Cleaning the Apical Third:
Adequate irrigation ideally should reach the apical part of the canal and interact with the walls. However, there are limitations on how safely and efficiently this could be achieved, especially in a curve and calcified canal. When using needle irrigation, the effectiveness of irrigation flow close to the apex is a function of the depth of insertion, the needle’s diameter, and the pressure produced by the clinician (3). A pressure difference is needed to make flow happen, and flow occurs from higher pressure to lower pressure—the more significant the difference, the greater the flow. The diameter of the needle also has an impact on the flow. It is recommended to choose a needle size which is appropriately matching to the size of the prepared root canal. It is also important to remember that the closer to the apex the needle is placed, the risk of hypochlorite extrusion through the apex is increased.
Hypochlorite accident, even though uncommon, is an unfortunate event. It is reported that it is more common in female patients probably because of the less thickness and density of the bone; it is also more common in maxillary and posterior teeth of the proximity to the buccal surface. Other anatomical factors, shown in 2 cases by CBCT imaging (Fig 1 and 2), have also been associated with these unfavorable events, such as fenestration or anatomic variation close to the tooth’s apex, causing communication of the apex with the vital structures. (4)
Sequence:
Different irrigation sequences are proposed in the literature. The different irrigating solutions may positively or negatively interact with each other. Therefore, adequate knowledge of the irrigant interaction is needed when combining solutions.
Sodium Hypochlorite should be used as a solvent of organic tissue throughout the cleaning and shaping procedure. However, during mechanical preparation, a smear layer is created, containing inorganic material and bacteria, where NaOCl alone could not be effective for its removal. A chelator, such as EDTA, would be recommended to eliminate the inorganic matter. Research shows that, in general, around 2 minutes is needed to eliminate the smear layer, but for the elimination of thicker layers, longer exposure time is needed. (5). It is becoming more accepted to remove the smear layer as it contains microbes and bacterial antigens, especially during instrumentation of necrotic cases. To benefit from the properties of both NaOCl and EDTA, it is important to know their interaction: ethylenediaminetetraacetic acid keeps its calcium-complexing ability when mixed with NaOCl. However, EDTA causes NaOCl to lose its tissue-dissolving ability. Clinically, this suggests that EDTA and NaOCl should be used separately. In case, an alternating irrigating regimen is chosen, abundant amounts of NaOCl should be administered to wash out remnants of the EDTA. It is also important to know that if Sodium Hypochlorite is used after EDTA, it could erode the dentin. This erosion may contribute to the weakening of the tooth structure, which may cause vertical root fracture. Paradoxically, this erosion may help in achieving cleaner walls in deeper aspects of dentin. (6, 13)
To overcome some of the mentioned problems, combinations of lower concentration of NaOCl with “soft” chelators are being proposed in the literature with some promising results. Etidronic acid or 1-hydroxyethane 1,1- diphosphonic acid (HEDP) was found to show short-term compatibility with NaOCl solutions at clinical strength, thus keeping the desired antimicrobial and proteolytic effects of NaOCl while adding an element of decalcification to the mixture. (7)
Proposed Protocol:
In general, Sodium Hypochlorite should be used throughout the cleaning and shaping procedure, understanding that the irrigant may not reach the full length of the canal at this time. If smear layer is created in isthmus areas EDTA can be added, again, knowing the limitation factors that this combination brings.
After the canal is shaped to the desired taper and apical size, NaOCl should be activated to promote flow of fresh solution into the untouched areas and to allow irrigants to interact with the walls and reach the apex. It is well known that taper and apical size influence the delivery of irrigation. The activation can be done with many different systems ranged from manual activation with a fitted gutta percha cone, to machine assisted devices (sonic, ultrasonic, multisonic, lasers, etc.).
It would be helpful to know that the choice of root filling sealer and the subsequent coronal restoration material may also play a role in choosing the final irrigation. For example, decalcifying materials should be used before resin, and bismuth-containing sealers while NaOCl is suggested to be used before bioceramic materials. Irrigation with chelators is recommended to remove the smear layer prior to use of dental adhesives for coronal restoration.
Advanced Technologies – Nanoparticles
Nanotechnology has been incorporated into Medicine successfully, and its use in dental field is being investigated in the recent years (14). In terms of disinfection of the root canal system, Chitosan nanoparticles have shown promising results with enhanced antibiofilm capability, and the potential to disable bacterial endotoxins. Nanoparticles have been added to intracanal medicaments and obturation sealers with promising results. They have also been suggested to be used as irrigation solutions, mainly for final irrigation of root canals as they are non-toxic to eukaryotic cells (15). Their usage is under extensive investigation.
Summary:
In summary, it is impossible to have one size fits all protocol in terms of disinfection. The irrigating protocol should be customized based on the clinical case. (8) For example, if we are working in a calcified canal, the use of alternating NaOCl and chelators can be beneficial. However, if the case has thin dentin walls and an open apex, this combination might not be the best choice since it may weaken the limited radicular dentin structure. If a pre-operative CBCT shows proximity to vital structures, caution in positioning of the irrigating needle need to be considered.
In conclusion, successful treatment does not necessarily mean sterilization of the root canal system but the reduction of the bacterial population to a subcritical level, which is compatible with healing. (9)
Figures:
Figure 1:
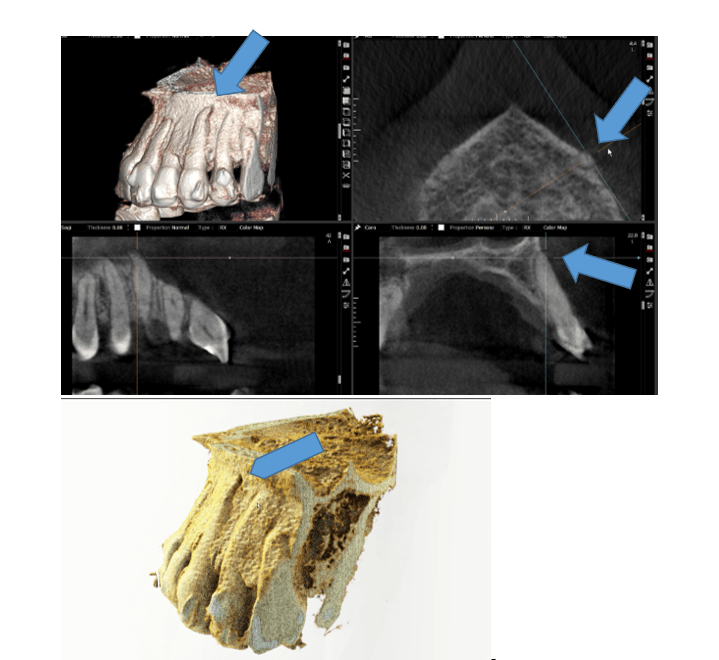
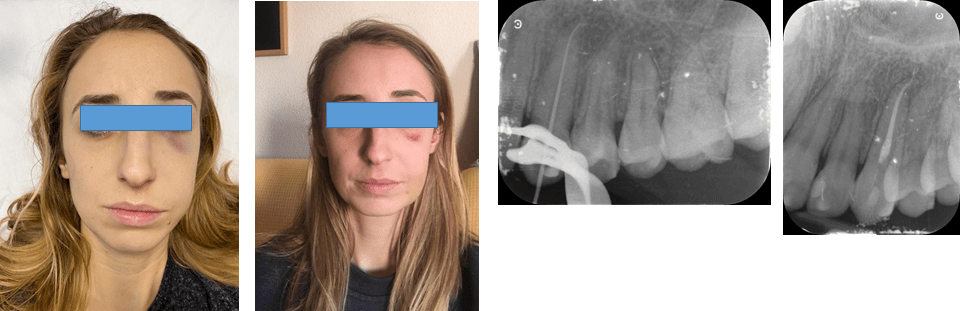
Sodium Hypochlorite accident on a female patient maxillary left canine. Note CBCT section showing no cortical bone in apex area after Invisalign orthodontic treatment. (Case courtesy of Dr. Sebastián Ortolani)
Figure 2:
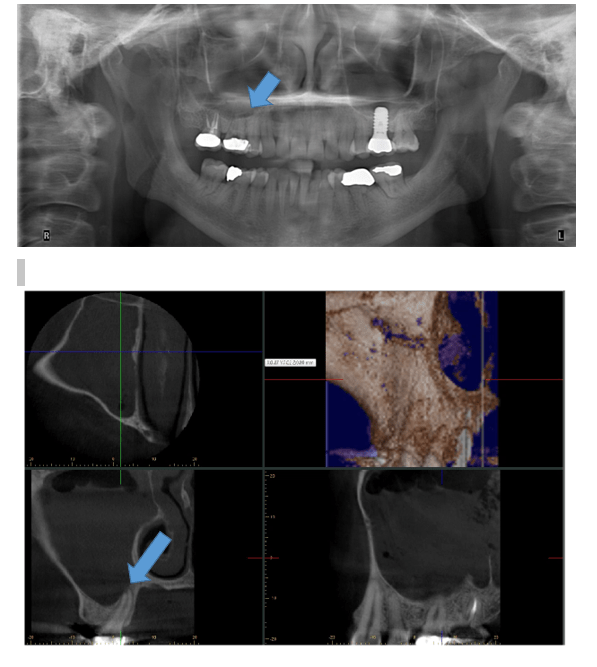
Sodium Hypochlorite in maxillary sinus because DB root connected directly to sinus. (Case provided by Dr. Bruno Azevedo)
References:
- Grossman LI, Meiman BW. Solution of pulp tissue by chemical agents. J Am Dent Assoc. 1941;28: 223–225.
- Basrani, B. and Haapasalo, M. (2012), Update on endodontic irrigating solutions. Endod Topics, 27: 74-102. https://doi.org/10.1111/etp.12031
- Chow TW. Mechanical effectiveness of root canal irrigation. J Endod. 1983 Nov;9(11):475-9. doi: 10.1016/S0099-2399(83)80162-9. PMID: 6586975.
- Zhu WC, Gyamfi J, Niu LN, Schoeffel GJ, Liu SY, Santarcangelo F, Khan S, Tay KC, Pashley DH, Tay FR. Anatomy of sodium hypochlorite accidents involving facial ecchymosis – a review. J Dent. 2013 Nov;41(11):935-48. doi: 10.1016/j.jdent.2013.08.012. Epub 2013 Aug 28. PMID: 23994710; PMCID: PMC3824250.
- Haapasalo, M., Shen, Y., Wang, Z. et al. Irrigation in endodontics. Br Dent J 216, 299–303 (2014). https://doi.org/10.1038/sj.bdj.2014.204
- WeiQianDDS, PhDYaShenDDS, PhDMarkusHaapasaloDDS, PhD Quantitative Analysis of the Effect of Irrigant Solution Sequences on Dentin ErosionJournal of Endodontics Volume 37, Issue 10, October 2011, Pages 1437-1441
- Grawehr, M., Sener, B., Waltimo, T. and Zehnder, M. (2003), Interactions of ethylenediamine tetraacetic acid with sodium hypochlorite in aqueous solutions. International Endodontic Journal, 36: 411-415. https://doi.org/10.1046/j.1365-2591.2003.00670.x
- Dotto L, Sarkis Onofre R, Bacchi A, Rocha Pereira GK. Effect of Root Canal Irrigants on the Mechanical Properties of Endodontically Treated Teeth: A Scoping Review. J Endod. 2020 May;46(5):596-604.e3. doi: 10.1016/j.joen.2020.01.017. Epub 2020 Mar 5. PMID: 32147184
- Siqueira JF, Jr., Rocas IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod. 2008; 34(11): 1291-301 e3.
- Prada I, Micó-Muñoz P, Giner-Lluesma T, Micó-Martínez P, Muwaquet-Rodríguez S, Albero-Monteagudo A. Update of the therapeutic planning of irrigation and intracanal medication in root canal treatment. A literature review. J Clin Exp Dent. 2019;11(2): e185-e193. Published 2019 Feb 1. doi:10.4317/jced.55560
- Sim, T.P.C., Knowles, J.C., Ng, Y.‐L., Shelton, J. and Gulabivala, K. (2001), Effect of sodium hypochlorite on mechanical properties of dentine and tooth surface strain. International Endodontic Journal, 34: 120-132. https://doi.org/10.1046/j.1365-2591.2001.00357.x
- Clegg M S, Vertucci F J, Walker C, Belanger M, Britto L R. The effect of exposure to irrigant solutions on apical dentin biofilms in vitro. J Endod 2006; 32: 434–437.
- Baumgartner J C, Mader C L. A scanning electron microscopic evaluation of four root canal irrigation regimens. J Endod 1987; 13: 147–157.
- Raura, N., Garg, A., Arora, A. et al.Nanoparticle technology and its implications in endodontics: a review. Biomater Res24, 21 (2020). https://doi.org/10.1186/s40824-020-00198-z
- Shrestha A, Kishen A. Antibiofilm efficacy of photosensitizer-functionalized bioactive nanoparticles on multispecies biofilm. J Endod. 2014 (40) 1604 – 1610.
Dr. Bettina Basrani is Tenured Associate Professor and Director, MSc Program in Endodontics at the Faculty of Dentistry, University of Toronto, Ontario, Canada. She serves as reviewer for several endodontic journals. Dr Basrani is a member of many endodontics societies around the world.
Dr. Gevik Malkhassian is a Specialist in Endodontics and an Assistant Professor at the Faculty of dentistry, University of Toronto. He is a fellow of The Royal College of Dentists of Canada. He serves as reviewer for a few endodontic journals. He has served as the president of OKU (An honorary dental Society) and the Endodontic Alumni association at the University of Toronto.