Broken Instruments – Clinical Decision Making Algorithm
 By Dr. Michael Solomonov
By Dr. Michael Solomonov
The fracture of endodontic instruments during root canal treatment is a complication every endodontist must have to deal with. The reported frequency rate for fractured instruments varies from 0.7% to 6% of cases.1 Stainless steel instrument fracture can be prevented mostly by discarding instruments that show signs of metal fatigue2 however, NiTi instrument separation can happen without any sign of fatigue.3-5 The single use of rotary NiTi instruments reduces the chance of breakage to 0.9% but does not prevent the chance of fracture entirely.6-7 Common reasons for fracture of rotary NiTi files are flexural and/or torsional fatigue.4,6 Unfortunately, it is theoretically impossible to create nonbreaking instruments because of the fact that more flexible instruments, that are more resistant to cyclic fatigue, have been assumed to be less resistant to torsional load and vice versa.8
The common approach for dealing with a broken instrument is its removal. The use of an operative microscope to facilitate canal widening to the level of the broken fragment and its removal by ultrasonic tips and/or some type of grasping equipment is accepted worldwide. 9
The rate of successful fragment removal is high 10 but can it be defined as endodontic treatment success? Immediate untoward results of dentin removal may be perforation or strip perforation at the danger zone 11. Removal of healthy dentin and especially peri-cervical dentin decreases root strength and can predispose the root to vertical root fracture 11-15 (Fig1).The first principle of medicine is do not hurt your patient, please remember it. The goal of endodontics is to treat or prevent apical periodontitis.16 The most common cause of periapical lesions is intra-radicular infection.17 A broken file by itself does not induce inflammation.18 We often see teeth with fractured instruments that were treated many years ago and have no clinical or radiologic signs of periapical inflammation (Fig 2). Periapical healing takes place if during Endodontic treatment disinfection decreases microbial load beneath the specific threshold.19 Nowadays, total sterilization of canals is still a utopic goal.19 If the broken instrument prevents effective disinfection and the apical lesion does not heal or a new lesion is developed, apical surgery can be used without sacrificing peri-cervical dentin.

Figure 1. VRF of Mesial root five years after retrieval of broken instrument
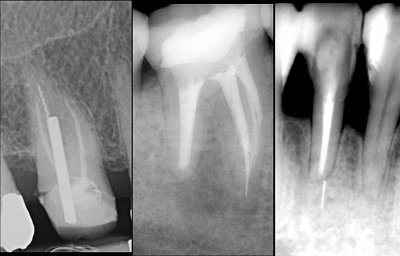
Figure 2. Normal apical tissue. Broken instruments are not a reason for apical periodontitis.
The proposed clinical algorithm is based upon the understanding of biological processes that are responsible for periapical lesions and tooth biomechanics. Its goal is the maintenance of a long-term functional tooth.18
If Instrument was broken in a canal with:
Vital Pulp (Not a heavily infected canal). Location of fragment can influence our decisions-
a. Instrument fractured in the apical part of the canal-
Removal of the fractured file fragment should not be attempted. One should change working length, prepare canal up to the fragment, use some type of NaOCl agitation and obturate the canal in the same visit (Figures 3).
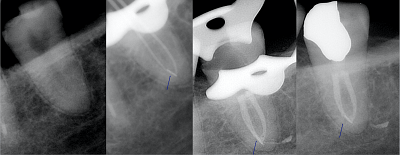
Figure 3. Irreversible pulpitis, broken fragment in apical part. Follow-up two years
b. Instrument fractured in the middle part of the canal-
One should try to bypass the broken instrument (Figures 4). If bypass is impossible, my recommendation is to obturate the canal up to the instrument; Follow-up is obligatory, and in case of post-treatment endodontic disease, apical surgery should be considered.
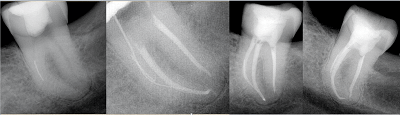
Figure 4. Irreversible pulpitis. Broken file in middle part of MB canal. Bypass with afterward hand files shaping up to #30. Fragment left in the canal.
c. Instrument fractured in coronal part of canal-
Removal of a fractured instrument should be attempted with minimal dentin removal, different types of grasping equipment can be used
Non Vital Pulp (An Infected Case)
The stage of shaping and cleaning at the moment of file breakage influences our decisions-
a. Instrument fractured after major cleaning and shaping- canal is prepared to at least size #30. Recommendations are the same as in vital pulp cases:
- Apical third of the canal: removal of the fractured file fragment should not be routinely attempted. Obturation up to the fragment is recommended.
- Middle part of the canal: one should try to bypass the broken instrument. If bypass is impossible, obturate canal up to instrument and follow up , apical surgery should be considered.
- Coronal part of the canal: removal of fractured instrument should be attempted with minimal dentin removal.
b. Separation of instrument before significant instrumentation and irrigation have been performed
- Bypass is highly recommended. Canal cross-section influences this procedure: Long oval and flattened canals and isthmuses enables this procedure, while round canal can impede it. If bypass was successful completion of shaping of the canal by hand files up to size #30 is recommended. Removal of the fragment is not necessary.
- If bypass was unsuccessful, inter-appointment medication with Ca(OH)2 for two – four weeks combined with NaOCl agitation is recommended for disinfection. After final obturation, follow-up is obligatory (Figures 5), and in case of post-treatment endodontic disease, apical surgery should be considered (Figures 6).
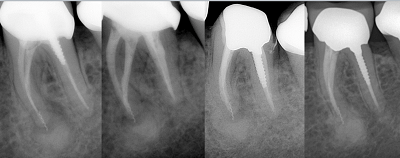
Figure 5. Apical periodontitis – two-visit retreatment with unsuccessful bypass of broken instrument in ML canal. Healing process after six months and healed lesion after seven years
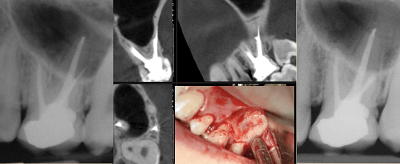
Figure 6. Symptomatic apical periodontitis. Broken instrument in apical part and in apical area of DB canal. Apical surgery. Image courtesy of Dr. Avi Hadad.
Successful removal of fractured instruments may risk the long-term outcome of the tooth by sacrificing sound peri-cervical dentin, which may lead to perforations and predispose the tooth to vertical root fracture. The clinician should consider the micro-biological and biomechanical aspects during clinical decision making.
References
- Spili P, Parashos P, Messer H. The impact of instrument fracture on outcome of endodontic treatment. J Endod 2005;31:845-850.
- Glickman GN, Dumsha TC. Problems in canal cleaning and shaping. In: Gutman L, Dumsha C, Lovdahl, Hovland E, editors. Problem Solving in Endodontics. 3rd Ed. St Louis (MO): C.V. Mosby; 1997. p. 91.
- Alapati SB, Brantley WA, Svec TA, Powers JM, Nusstein JM, Daehn GS. SEM observations of nickel-titanium rotary endodontic instruments that fractured during clinical use. J Endod 2005;31:40–43.
- Parashos P, Gordon I, Messer HH. Factors influencing defects of rotary nickel-titanium endodontic instruments after clinical use. J Endod 2004; 30:722–725.
- Pruett JP, Clement D J, Carnes DL Jr. Cyclic fatigue testing of NiTi endodontic instruments. J Endod 1997;23:77-85.
- Arens FC, Hoen MM, Steiman HR, Dietz GC, Jr. Evaluation of single-use rotary nickel-titanium instruments. J Endod 2003;29:664–666.
- Caballero‐Flores H, Nabeshima CK, Binotto E, Machado ME. Fracture incidence of instruments from a single‐file reciprocating system by students in an endodontic graduate programme: a cross‐sectional retrospective study. International endodontic journal. 2019 Jan;52(1):13-8.
- Zhou HM, Shen Y, Zheng W, Li L, Zheng YF, Haapasalo M. Mechanical properties of controlled memory and superelastic nickel-titanium wires used in the manufacture of rotary endodontic instruments. Journal of endodontics. 2012 Nov 1;38(11):1535-40.
- Ruddle CJ. Micro-endodontic nonsurgical retreatment. Dent Clin North Am 1997; 41:429–454.
- Nevares, G., Cunha, R.S., Zuolo, M.L. and da Silveira Bueno, C.E., 2012. Success rates for removing or bypassing fractured instruments: a prospective clinical study. Journal of endodontics, 38(4), pp.442-444.
- Souter NJ, Messer HH. Complications associated with fractured file removal using an ultrasonic technique. J Endod 2005;31: 450-452.
- Sornkul E, Stannard JG. Strength of roots before and after endodontic treatment and restoration. J Endod 1992;18:440 –443.
- Clark D, Khademi J, Herbranson E. Fracture resistant endodontic and restorative preparations. Dent Today 2013;32:118,120-3.
- Stress distribution in a mandibular premolar after separated nickel-titanium instrument removal and root canal preparation: a three-dimensional finite element analysis. Ni, N., Ye, J., Wang, L., Shen, S., Han, L., & Wang, Y. Journal of International Medical Research,(2019). 47(4), 1555-1564.
- Fu M, Huang X, Zhang K, Hou B. Effects of ultrasonic removal of fractured files from the middle third of root canals on the resistance to vertical root fracture. Journal of Endodontics. 2019 Nov 1;45(11):1365-70.
- Sundqvist G, Figdor D, Ørstavik D, Ford TP. Essential endodontology. Prevention and treatment of apical periodontitis. 1998.
- Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol 1965;20:340–349.
- Solomonov M, Webber M, Keinan D. Fractured endodontic instrument: a clinical dilemma. Retrieve, bypass or entomb?. The New York state dental journal. 2014;80(5):50-2.
- Siqueira Jr, José F., and Isabela N. Rôças. “Clinical implications and microbiology of bacterial persistence after treatment procedures.” J Endod 34.11 (2008): 1291-1301.
Michael Solomonov, D.M.D., is a board-certified endodontist and the director of the Postgraduate Endodontic program in Endodontics at the Sheba Medical Center, Tel-Hashomer, IDF, Israel .