Flowcharting of the Proposed Clinical Decision-Making Algorithm of Broken Endodontic Instruments: Decision-making to Retrieve, Bypass, or Entomb
By Drs. Nurcan Deniz and Ekim Onur Orhan
Clinical approaches have been described to accessing fractured instruments, depending on their location in the canal and stage of cleaning and shaping (1-3). In the case of root canal instrument fracture, the practitioner has to be well-educated to control the unfortunate situation. The clinical decision-making should be evidence-based on the information of the corresponding success rates of each treatment option, evaluated through potential risks of ‘removal’ versus ‘leaving in situ’ (3).
For clinicians, evaluating the multiple scenarios of broken canal instruments is not only hard but also might be led to confusion in the assessment of the alternatives (4). Very recently, Solomonov (5) has proposed a “clinical algorithm based upon the understanding of biological processes that are responsible for periapical lesions and tooth biomechanics”. In this context, the proposed algorithm has been well-described with the sections in the paper (5).
To achieve a better understanding of the proposed algorithm by Solomonov (5), the codes of the algorithm should be resolved for clinicians. More specifically, the main goal of the paper is to represent the proposed complex algorithm by Solomonov (5) with an evidence-based flowchart. The flowchart was drawn by the vector diagram using Microsoft Visio (v15.0.4623.1000; Microsoft Corp., Redmond WA) (Figure 1). There were four symbols used in the flowchart of assembly language programs: process, decision, terminal, and flowlines. Accordingly, the “rectangular” frame indicates the “process” of any type of internal operation inside the processor or memory, the “rhombus” frame indicates the “decision”. The “ellipse” frame indicates the “terminal” that of the starting or end of the process, or interrupt program. The ‘flowlines’ show the direction of flow.
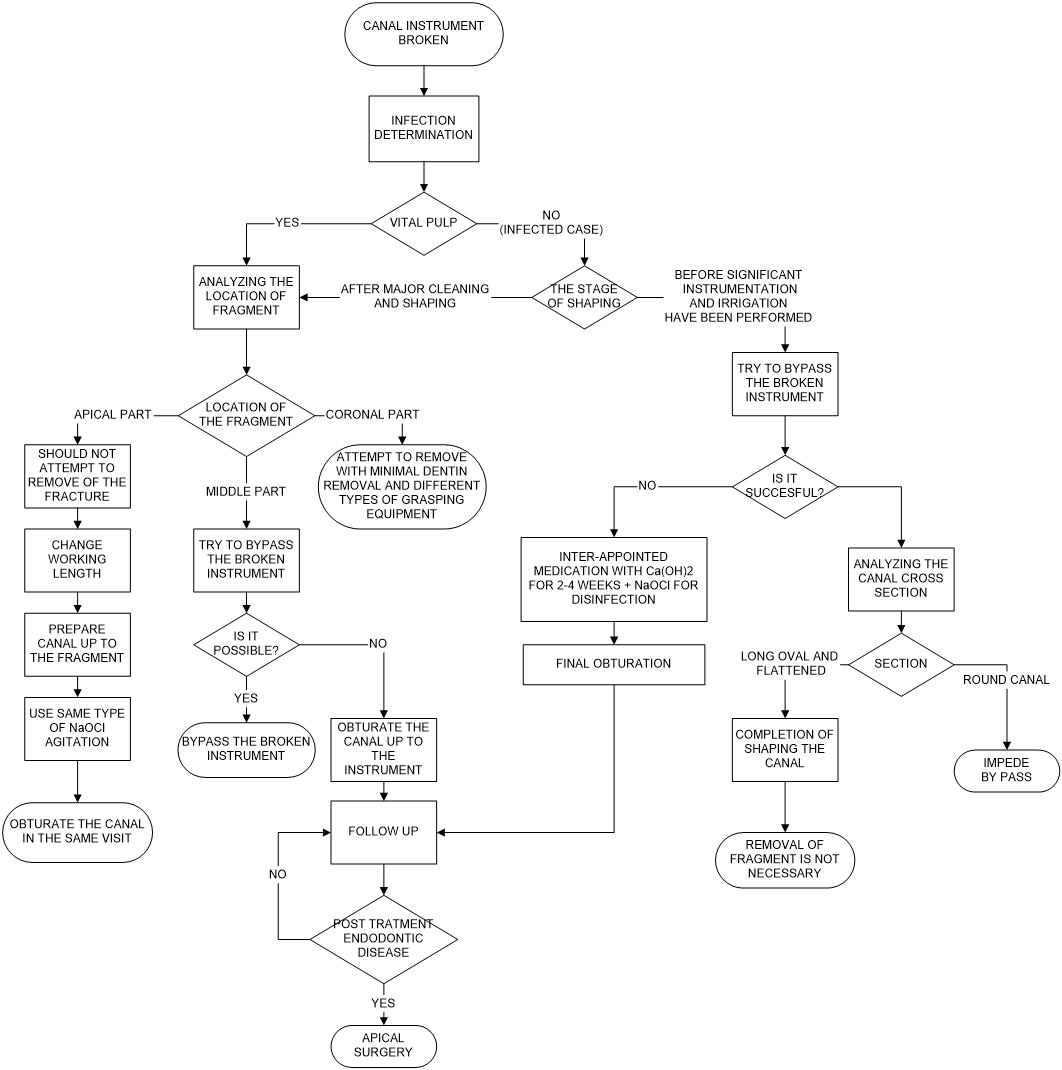
Figure 1: The flowchart transitions of the proposed algorithm (5).
References
1- Suter B, Lussi A, Sequeira P. Probability of removing fractured instruments from root canals. Int Endod J. 2005 Feb;38(2):112-23. doi: 10.1111/j.1365-2591.2004.00916.x.
2- McGuigan MB, Louca C, Duncan HF. Clinical decision-making after endodontic instrument fracture. Br Dent J. 2013 Apr;214(8):395-400. doi: 10.1038/sj.bdj.2013.379.
Ruddle CJ (2003) Removal of broken instruments. Endodontic Practice 6, 13–9.
3- Solomonov M, Webber M, Keinan D. Fractured Endodontic Instrument: A Clinical Dilemma Retrieve, Bypass or Entomb? J Mich Dent Assoc. 2015 Sep;97(9):44-6.
4- Dahlström L, Lindwall O, Rystedt H, Reit C. ‘Working in the dark’: Swedish general dental practitioners on the complexity of root canal treatment. Int Endod J 2017;50:636-645. https://doi.org/10.1111/iej.12675
5- Solomonov M, Broken Instruments – Clinical Decision Making Algorithm. PROBLEM SOLVING IN ENDODONTICS. NOVEMBER 2, 2020 URL: https://www.aae.org/specialty/communique/broken-instruments-clinical-decision-making-algorithm/
Dr. Nurcan Deniz: Department of Business Administration, Faculty of Economics and Administrative Sciences, Eskişehir Osmangazi University, 26040 Eskişehir, Turkey.
Dr. Ekim Onur Orhan: Department of Endodontics, Faculty of Dentistry, Eskişehir Osmangazi University, 26040 Eskişehir, Turkey; Translational Medicine Research and Clinical Center, Eskisehir Osmangazi University, 26040 Eskisehir, Turkey; Computer-Aided Diagnosis and Treatment Application and Research Center in Healthcare, Eskisehir Osmangazi University, 26040 Eskisehir, Turkey. Dr. Orhan can be reached at ekimonurorhan@gmail.com.